Disordered Eating in High Performance Sport
Introduction and Definitions
The Australian Institute of Sport (AIS) and National Eating Disorders Collaboration (NEDC) position statement on disordered eating in high performance sport.
The Australian Institute of Sport (AIS) is Australia’s peak high performance sport agency. The National Eating Disorders Collaboration (NEDC), an initiative of the Australian Government Department of Health, promotes nationally consistent, evidence-based responses to Disordered Eating (DE) and Eating Disorders (ED) in Australia. Both organisations are committed to ensuring the safety and welfare of all high performance athletes.
The AIS and NEDC have collaborated to provide these guidelines for athletes, coaches, support staff, clinicians and sporting organisations. The guidelines support the prevention and recognition of DE, and promote early intervention to optimise nutrition for performance in a safe, supported, purposeful and individualised manner. This position statement is a call to action to all involved in sport to be aware of poor self-image and poor body image among athletes. Sporting organisations should develop sport-specific positions and guidelines that foster a healthy sport system for athletes. The practical recommendations in this document are intended to guide the clinical management of DE in Australian high performance sport, putting in place a core multidisciplinary team (CMT) comprised of doctor, sports dietitian and psychologist. The clinical treatment and management of EDs is outside the scope of this document. There are further resources available in the National Practice Standards for Eating Disorders1 , the Royal Australian and New Zealand College of Psychiatrists clinical practice guidelines for the treatment of EDs (2014)2 and the UK National Institute for Health and Care Excellence guideline on EDs Recognition and Treatment (2017).3 In addition, the Australia and New Zealand Academy for Eating Disorders clinical practice and training Standards are due for publication in 2020.4-6
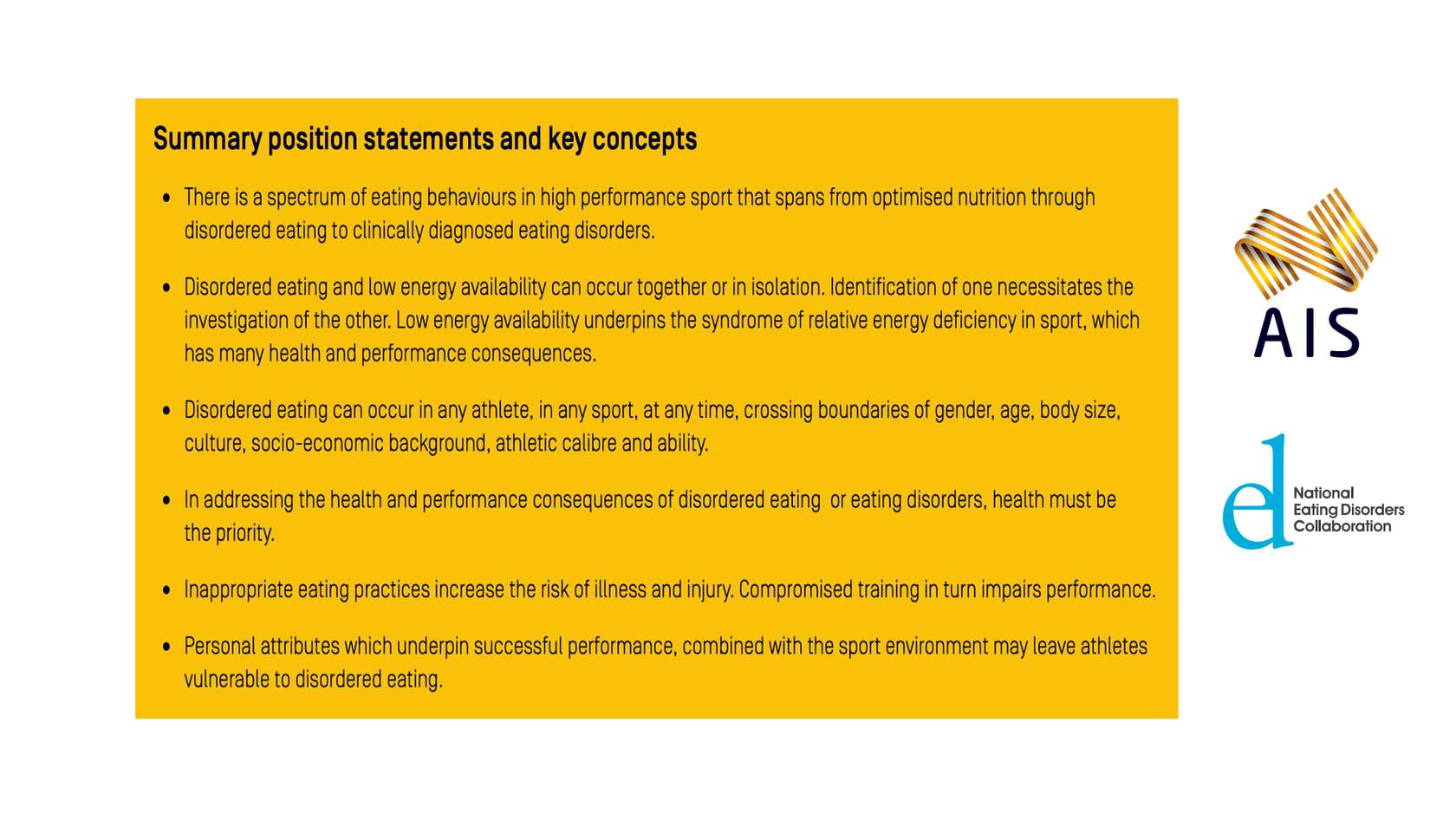
This document contains detailed discussion of each of the key themes of Background, Assessment, Prevention, and Creating A Healthy Sport System. Key position statements and concepts arising from this material are highlighted throughout the document in break-out boxes. A summary of all position statements and key concepts can be found at the end of Part Four.
Definitions
Organisations and Teams
Australian Institute of Sport (AIS)
The Australian Institute of Sport is Australia’s peak high performance sport agency. The AIS leads and enables a united and collaborative high performance sport system that supports Australian athletes to achieve international podium success.
National Eating Disorders Collaboration (NEDC)
The National Eating Disorders Collaboration is an initiative of the Australian Government Department of Health that develops a nationally consistent, evidence-based approach to the prevention and management of eating disorders in Australia.
Core Multidisciplinary Team (CMT)
A team of professional practitioners (doctors, dietitians, psychologists) who collaborate in the management of disordered eating cases. In the Australian case this would be a sports doctor or general practitioner, an accredited sports dietitian and a registered psychologist or endorsed sport psychologist.
High Performance Athlete
A high performance athlete is considered to be any athlete within the Australian performance pathway ranging from junior and senior elite level and including para and able-bodied athletes. From here on the high performance athlete will be referred to as the athlete.
Dietary and Eating Terms
Optimised Nutrition
Optimised nutrition involves a safe, supported, purposeful and individualised approach. It promotes healthy body image and thoughts about food, and is adaptable to the specific and changing demands of an athlete’s sport.
Energy Availability (EA)
Energy availability is the amount of energy that is available to support the body’s activities for health and function once the energy commitment to exercise has been subtracted from dietary energy intake. Energy availability = (Energy intake – Energy cost of exercise)/Fat free mass.
Low Energy Availability (LEA)
LEA occurs when there is a mismatch between energy intake and exercise load, leaving insufficient energy to cover the body’s other needs. It may arise from inadequate energy intake, increased expenditure from exercise, or a combination of both; and is either advertent or inadvertent.
Relative Energy Deficiency in Sport (RED-S)
RED-S is the syndrome of impaired physiological function including, but not limited to, metabolic rate, menstrual function, bone health, immunity, protein synthesis, cardiovascular health that arises from low energy availability.
Eating disorder (ED)
A serious, but treatable mental illness with physical effects that can affect any individual. Feeding and eating-related disorders are defined by specific criteria published in American Psychiatric Association’s (2013) Diagnostic and Statistical Manual of Mental Disorders (5th edition, DSM-5) which include problematic eating behaviours, distorted beliefs, preoccupation with food, eating and body image, and result in significant distress and impairment to daily functioning (e.g., sport, school/ work, social relationships)
Avoidant Restrictive Food Intake Disorder
A new DSM-5 diagnosis previously referred to as “Selective Eating Disorder.” ARFID is similar to anorexia in that both disorders involve limitations in the amount and/ or types of food consumed, but unlike anorexia, ARFID does not involve any distress about body shape or size, or fears of fatness.
Anorexia Nervosa
Characterized by weight loss (or lack of appropriate weight gain in growing children); difficulties maintaining an appropriate body weight for height, age, and stature; and, in many individuals, distorted body image.
Bulimia Nervosa
Characterised by a cycle of binge eating and compensatory behaviours such as self-induced vomiting designed to undo or compensate for the effects of binge eating.
Binge Eating Disorder
Characterized by recurrent episodes of eating large quantities of food (often very quickly and to the point of discomfort); a feeling of a loss of control during the binge eating episode; experiencing shame, distress or guilt afterwards; and not regularly using unhealthy compensatory measures (e.g., purging) to counter the binge eating.
Other Specified Feeding or Eating Disorders (OSFED)
An eating disorder classification used when all required criteria for a diagnosis have not been met but are problematic for health and daily functioning. OSFED includes five categories: Atypical Anorexia Nervosa, Bulimia Nervosa (of low frequency and/ or limited duration), Binge Eating Disorder (of low frequency and/or limited duration), Purging Disorder, and Night Eating Syndrome. All of these may be particularly relevant for athletes who are not underweight and/or where episodes of bingeing or compensatory behaviours are less frequent than required for a diagnosis.
Other Conditions;
Disordered eating (DE)
Disordered eating is any eating behaviour that is not optimised. DE may range from what is commonly perceived as normal dieting to reflecting some of the same behaviour as those with eating disorders, but at a lesser frequency or lower level of severity
Orthorexia
Obsession with proper or ‘healthful’ eating. Although being aware of and concerned with the nutritional quality of the food eaten isn’t a problem in and of itself, people with orthorexia become so fixated on so-called ‘healthy eating’ that they actually damage their own well-being.
Atypical Anorexia Nervosa
Atypical anorexia includes those individuals who meet the criteria for anorexia but who are not underweight despite significant weight loss. Research studies have not found a difference in the medical and psychological impacts of anorexia and atypical anorexia. Even if all the DSM-5 criteria for anorexia are not met, a serious eating disorder can still be present. This is an OSFED presentation that may be easily masked in the HP sports context but which presents serious risk.
Disordered Eating in Athletes
"Disordered eating in an athlete sits on a spectrum between optimised nutrition and an eating disorder"
DE in an athlete sits on a spectrum between optimised nutrition and an ED (Figure 1). An individual with DE may regularly engage in behaviours such as skipping meals, compulsive eating, compulsive exercise and/or restrictive eating but without meeting all required criteria for an ED. Both DE and dieting behaviour are common indicators for developing an ED.7 10 The 2019 International Olympic Committee (IOC) consensus statement on mental health in elite sport compares characteristics of ED versus DE (Table 1.)11 DE may involve short-term restrictive diets, which progress to chronic energy or nutrient restriction, binge eating, active and passive dehydration, use of laxatives, diuretics, vomiting, and diet pills with or without excessive training. Individual athletes can move back and forth along the spectrum of eating behaviour at any point in time over their career and within different stages of a training cycle (e.g. during the off-season, pre-season, when injured). Athletes are more likely to present with DE than a clinical ED.11 12 13 However, there are health and performance implications regardless of where an athlete falls along the spectrum, and risks increase when DE worsens into a diagnosable ED. Behaviour that was previously ‘encouraged and rewarded’ such as losing weight to enhance performance, may result in a failure to maintain adequate energy availability required for training and competition demands. These behaviours may not have been maladaptive at first, but may develop into problematic eating behaviour and worsen to reflect ED psychopathology. Familiarisation with ED diagnostic criteria among members of an athlete’s support network facilitates appropriate questions about eating behaviour. The associations between body composition manipulation, EA, nutrition, psychosocial status, body image, health and performance are complex.14 Evaluation and management requires a professional and cohesive team.
Figure 1: The spectrum of eating behaviour in the high performance athlete from optimised nutrition to disordered eating to eating disorders.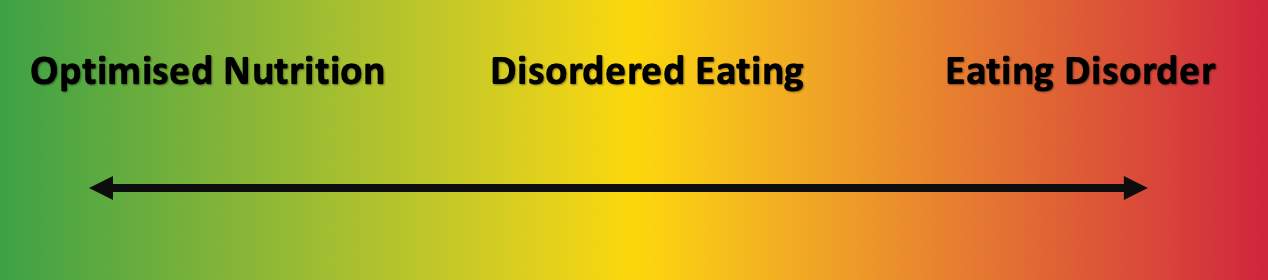
Optimised Nutrition
Safe, supported, purposeful and individualised nutrition practices that best balance health and performance
Disordered Eating
Problematic eating behaviour that fails to meet the clinical diagnosis for an eating disorder
Eating Disorder
Behaviour that meets DSM-5 diagnostic criteria for a feeding and eating disorder
Table 1: Characteristics of eating disorders versus disordered eating in elite athletes – reprinted with permission from The IOC Consensus Statement on Mental Health in Elite Sport (Reardon et al. 2019).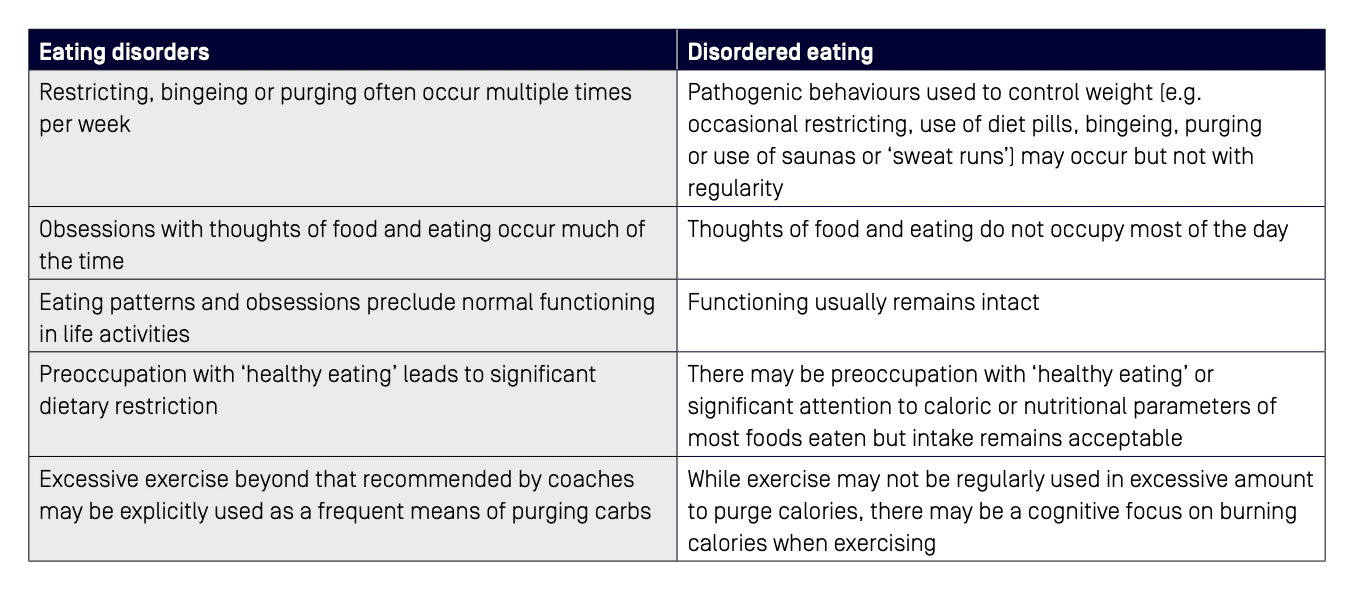
Reprinted with permission from The IOC Consensus Statement on Mental Health in Elite Sport (Reardon et al. 2019).
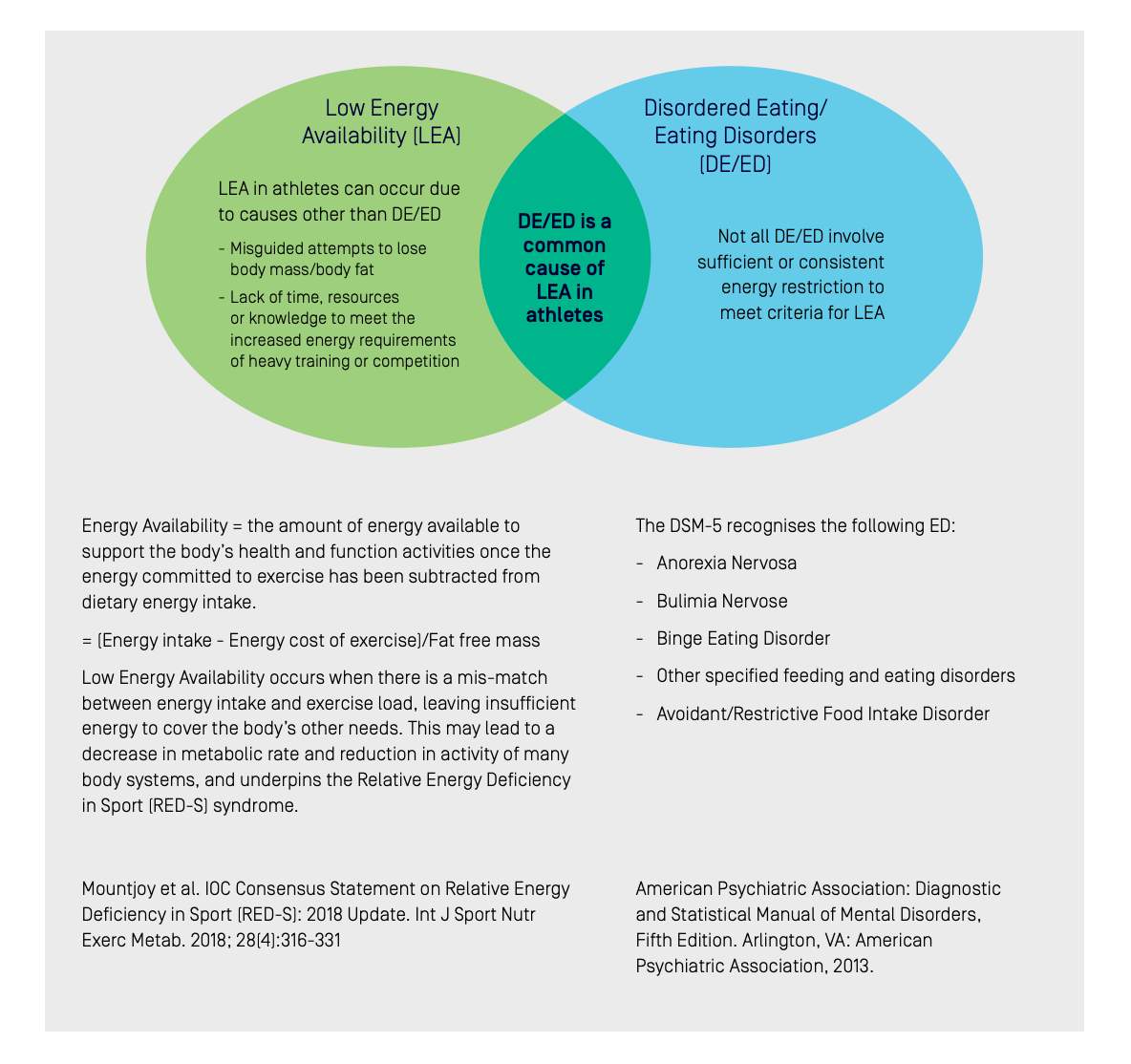
DE and low energy availability (LEA) can occur together, or in isolation (see Figure 2). Identification of one necessitates the investigation of the other. LEA may be difficult to recognise since an athlete may be stable in weight but deficient in energy.14 The assessment of energy availability (EA) is complicated by errors in the measurement of its component parts and failure to account for other factors such as dietary quality and within-day energy spread.15 Added complexity in working with athletes comes from sport-specific pressures and individual comorbidities as well as cultural, familial, individual, and genetic/ biochemical factors.16 As shown in Figure 2, DE may exist with or without low energy availability , which underpins the syndrome of Relative Energy Deficiency in Sport (RED-S) as described by an expert panel of the International Olympic Committee.
Figure 2: Eating disorders/disordered eating can occur in the absence or presence of low energy availability.
Health and Performance Consequences of Disordered Eating Behaviour
"Inappropriate eating practices can have detrimental effects on sports performance"
In addressing the health and performance consequences of DE or an ED, health must be the priority. Inappropriate eating practices can have detrimental effects on sports performance. One of the health risks of DE or EDs is the potential development of relative energy deficiency in sport (RED-S).7 In addition to the direct impairment of physiological and psychological function, DE can increase the risk of illness and injury, compromise training quality and consistency and indirectly interfere with competition goals.16 If DE is in conjunction with LEA, there may be suppression of physiological processes, resulting in impairments of bone health, menstrual function, endocrine, metabolic and hematological status, growth and development, psychological well-being, and cardiovascular, gastrointestinal and immunological systems (Figure 3A).
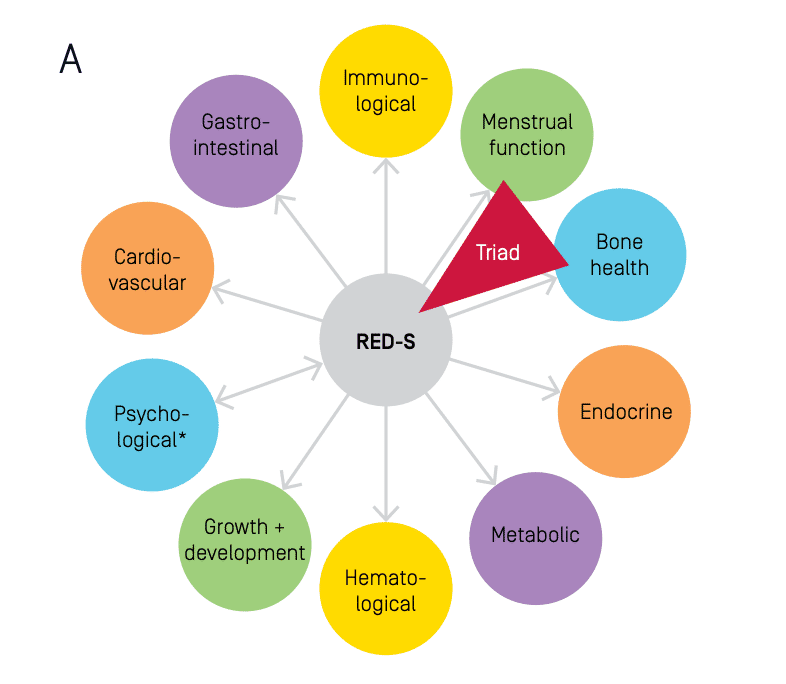
Figure 3A: Health Consequences of Relative Energy Deficiency in Sport (RED-S) showing expanded concept of The Triad to acknowledge a wider range of outcomes and the application to male athletes (*Psychological consequences can either precede RED-S or be the result of RED-S).
The long-term consequences of LEA are particularly critical to the adolescent athlete, affecting the accrual of peak bone mineral density (BMD) and stature, neurological18 and reproductive system development.14 Even without LEA, there may be other consequences of DE behaviours including electrolyte imbalances, dehydration, nutritional deficiencies, gastrointestinal problems (dental, gingival, bleeding, ulceration, bloating, constipation) and mental health issues (depression, anxiety, personality disorders, substance abuse, self-harm and suicidal ideation).19
When starved of energy, the body responds by reducing its metabolic rate. Since the human brain operates at a very high metabolic rate, and uses a substantial portion of total energy and nutrient intake,20 the brain is particularly vulnerable to inadequate fuel for its brain function.21 A person with DE may struggle to make decisions, solve problems and regulate their emotions.22 Restricted eating, malnourishment, and excessive weight loss can lead to changes in brain chemistry, resulting in increased symptoms of depression and anxiety.23 All of these may affect the athlete’s performance, their ability to engage in day-to-day tasks, their capacity for insight into problems associated with their eating, and their ability to engage with psychological treatments.
Performance consequences (Figure 3B) of DE may arise from interrupted or less effective training (e.g. increased illness and injury, reductions in training capacity, recovery and adaptation) as well as acute impairments on competition day from inadequate fueling for the event (e.g. reduction in co-ordination, concentration, mood, strength and endurance).16 Studies using different methodologies across different sports have reported detriments to performance due to persistent energy deficiency, which may or may not encompass DE. For example, elite male and female distance runners with markers of LEA reported 4.5 times more bone injuries and a 10-fold increase in missed training days due to injury, compared to those with normal EA.
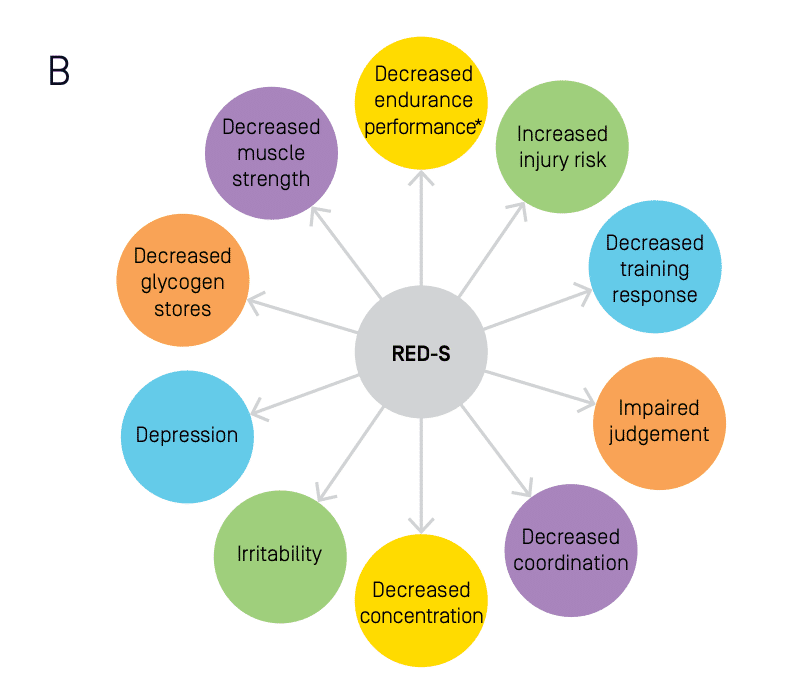
Figure 3B: Potential Performance Effects of Relative Energy Deficiency in Sport (*Aerobic and anaerobic performance). (Reproduced from reference)
Meanwhile, a cross-sectional survey of 1000 female athletes across a range of sports found increased odds of performance impairments (decreased training response, impaired judgement, decreased coordination, decreased concentration, irritability, depression and decreased endurance performance) in those judged to have LEA.25 Separate longitudinal investigations of elite female endurance athletes showed a reduction in maximal aerobic capacity and running speed after just two months of LEA, while swimmers with LEA demonstrated a 10% decrease in speed during a 400 m time trial after a 12 week training block in contrast to an 8% increase in performance noted in those with adequate EA.
Prevalence and Contributing Factors to Disordered Eating in Athletes
"Disordered eating can occur in any athlete, in any sport, at any time, crossing boundaries of gender, age, body size, culture, socio-economic background, athletic caliber and ability"
DE can occur in any athlete, in any sport, at any time, crossing boundaries of gender, age, body size, culture, socio-economic background, athletic caliber and ability. The estimated prevalence of DE and/or ED in athletes ranges from 0 – 19% in males and 6 – 45% in females.11 Overall, there is a higher prevalence of DE and EDs in athletes compared to non-athletes27 but sport-specific demands and individual characteristics of the athlete lead to a wide variation in prevalence of DE and ED across different sports.17 Much of the prevalence data regarding DE in athletes originates from studies of Scandinavian cohorts and North American collegiate athletes, predominantly featuring Caucasian and able-bodied populations.7 28 There is a paucity of prevalence data in para-athletes with further research and understanding required to adequately address and inform best practice in this population.29 An environment in which there is pressure to either lose or gain weight and/or to maintain meticulous control of body composition may contribute to an increased prevalence of DE and ED's. Athletes may be underweight, normal weight or overweight, irrespective of DE or EDs.30 Personal attributes and pressures for athletes which underpin successful performance, such as perfectionism or obsessive traits, combined with the sport environment may leave athletes vulnerable to DE.
Higher Risk Sports
Three categories of sports, defined as aesthetically judged, gravitational and weight class, are consistently identified as high risk for the development of DE and EDs (Table 2).14 Successful performance in these sports generally involves individual, or combinations of, features such as low body mass, leanness, high power: weight ratio, subjective judgements on appearance and rapid weight loss for weigh-ins. It should be remembered however that athletes are at risk of DE and ED across all sports and these high-risk categories are neither exclusive nor exhaustive. Risk factors for DE and EDs in high performance athletes can be seen in Table 3.
Table 2: Weight sensitive sports classified into three main groups at risk for decreased EA.
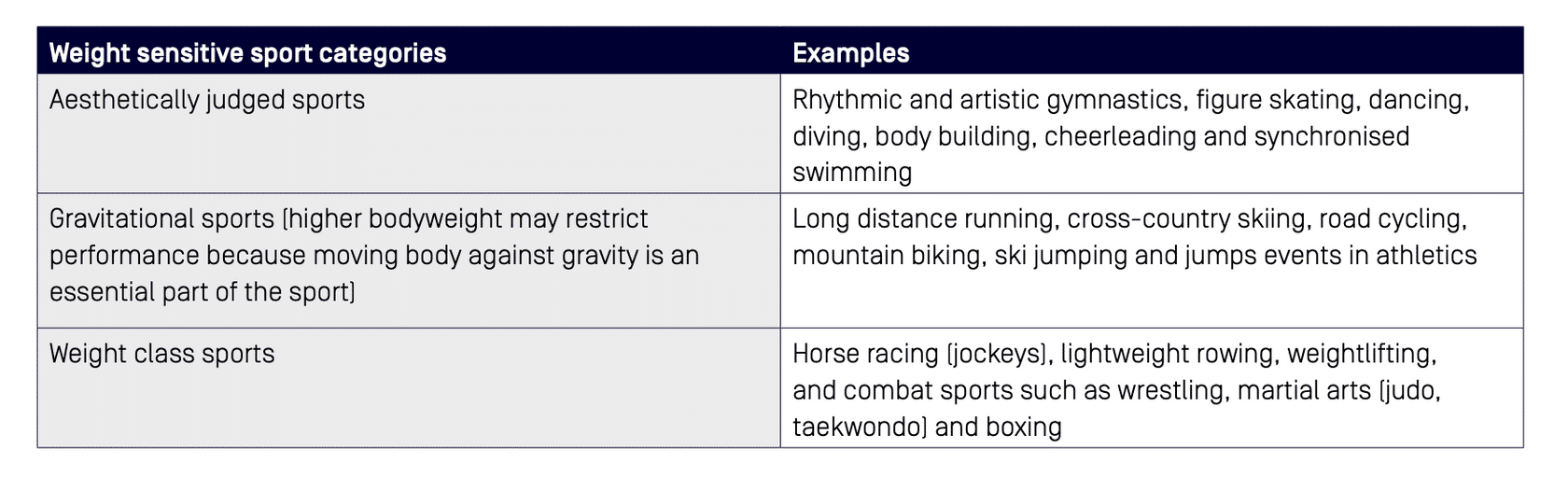
Table 3: Risk factors for disordered eating and eating disorders in high performance athletes.
Biological Risk Factors
- Age
- Stages of growth, development or puberty
- Genetic risk factors e.g. ED, addictions in family
- Precocious growth or development
- Growth or development that is significantly different from the average
Psychological Risk Factors
- Body dissatisfaction, body image distortion
- Low self-esteem
- Personality traits e.g. perfectionism
- Obsessive-compulsive tendencies/traits
- Neuroticism (depression, anxiety, emotional lability)
- Harm avoidance
- Heightened stress reactivity
- Inflexible, rule-drive, drive for order and symmetry
- Risk taking behaviour
Socio-cultural Risk Factors
- Eating pressures/modelling
- Peer pressure re: physical appearance or weight
- Influence of the media
- ‘Thin ideal’, ‘muscularity ideal’ or ‘fit ideal’
- Direct or perceived pressure to modify appearance or weight
- Weight/appearance-based teasing, bullying
- Social isolation
- Experiences of weight stigma, including in health care and within sporting environments
Sport-specific Risk Factors
- Transition periods: - Early start of sport-specific training - Making a senior team at a young age - Retirement (forced or voluntary) - Non-selection or de-selection - Injury, illness, surgery, time away from sport and training
- Changes in weight/body shape following injury/illness
- Pressures (perceived or real) to change body shape or composition
- Weight cycling
- Patterns of restriction or disordered behaviours
- Coaching behaviour and accepted ‘norms’ within sport
- Rules and regulations in sports
- Performance optimisation pressure
- Use of supplements, nutritional and ergogenic aids
- Body composition testing, weighing and measuring
- Public displays of ‘results’ in common areas e.g. training environment
- Media and social media pressure (perceived or real) to look a certain way
Gender-based Factors
- Media driven gender stereotypes
- Drive for muscularity/leanness/thinness
- Anabolic-androgenic steroid use
- Gender diversity
Other Risk Factors
- Chronic disease related to caloric utilisation e.g. diabetes, thyroid
- Co-occurring conditions e.g. Coeliac disease, other gastrointestinal conditions
- Para athletes
- LGBTQI+
- History of trauma
- History of food insecurity
- Major life transitions e.g. moving away from home, moving between schools, moving overseas
Early Identification of Disordered Eating
"Everyone in the sport system has a role to play in recognition and early intervention, and anyone can refer athletes to, and/or consult with, any member of the core multidisciplinary team"
DE in athletes can occur at any time; both precipitating, or being precipitated by, challenges in the athlete’s life as well as occurring during a time of successful performance.27 DE may manifest in a variety of ways that are unique to the individual. Rapport between the athlete and service provider, or knowledge of the athlete’s baseline health and function can be helpful in the identification of DE and EDs. While there is a growing openness and support for mental health concerns in elite sport,11 35 barriers to early identification and treatment of DE and ED still exist. 11 13 36 Athletes’ shame, stigma and fear of discrimination prevent them from disclosing problematic behaviour and seeking help, whereas limited knowledge about ED symptoms and reluctance to ask specifically about eating problems inhibit providers’ detection of DE and ED.37 It is widely accepted that the early identification and appropriate management of DE leads to better outcomes.38 EDs have one of the highest mortality rates amongst all mental illness, which underscores the importance of prevention efforts, timely detection and specialised treatment.39
Everyone in the sport system has a role to play in recognition and early intervention (‘early identifiers’), and anyone can refer athletes to, and/or consult with, any member of the CMT (doctor, sports dietitian and psychologist) for further assessment and support.19 Rapport between the athlete and his or her support network (coach, training partners or teammates, service providers) is important in recognising and evaluating DE and EDs.19 It is important for all personnel involved in the sport to be aware of the risk factors and warning signs or red flags of DE and EDs (see Tables 3 and 4). Personnel should also be informed of effective communication channels for concerns. Some warning signs (Table 4) can occur early (behavioural changes) whereas others such as weight changes may occur later in the person’s trajectory of DE.
Periodic evaluation can assist with early recognition of athletes who may be at risk and/or are exhibiting early signs of DE. Steps can then be taken to mitigate risk and prevent development of an ED. The goals of assessment are to identify DE or EDs, investigate the presence of LEA/RED-S and its consequences, and manage acute and chronic complications in the athlete. Evaluation should include nutritional, physical and psychological parameters. Where DE behaviours are recalcitrant and/or when an ED is detected, care involves complex, coordinated management of acute and chronic complications. Referral for specialised medical treatment, external to the National Sporting Organisation (NSO), National Institute or Academy of Sport, club or other performance environment, is advised.
Table 4: Warning signs or red flags for disordered eating and eating disorders in athletes.
- Preoccupation with food, calories, body shape and weight
-
Polarised/dichotomous thinking (including but not limited to thoughts about food, body or exercise)
-
Avoidance of food-related social activities
-
Restrictive eating e.g. cutting down or cutting out food groups, nutrients, reducing overall energy intake, counting, measuring and weighing food
-
Bathroom visits after meals
-
Evidence of binge eating (large amounts of food purchased/consumed, evidence of food wrappers hidden in the bin or another location)
-
Restriction followed by binge eating
-
Secretive behaviour regarding food intake and/or exercise behaviour
-
Increasing rigid or inflexibility in situations

-
Wearing baggy or layered clothing that hides body shape
-
Relentless, excessive exercise
-
Exercise through injury/illness with inadequate recovery
-
Bone stress injury
-
Hormone dysfunction (including dysregulated menstrual cycle, libido & erectile function)
-
Frequent illness
-
Low body fat
-
Dehydration
-
Bad breath, sore gums or signs of enamel loss on teeth
-
Swelling around jaw
-
Skin effects, including dry skin, fine hairs growing around the face, or signs of calluses on the knuckles
-
Unexpected weight gain beyond that expected from growth/development/puberty
-
Dramatic or rapid weight loss or gain or fluctuation
-
Persistent and/or problematic poor mental health
-
Increased attention to and/or criticism of one’s body
-
Feeling out of control in regards to food
-
Body image dissatisfaction and distortion
The Core Multidisciplinary Team
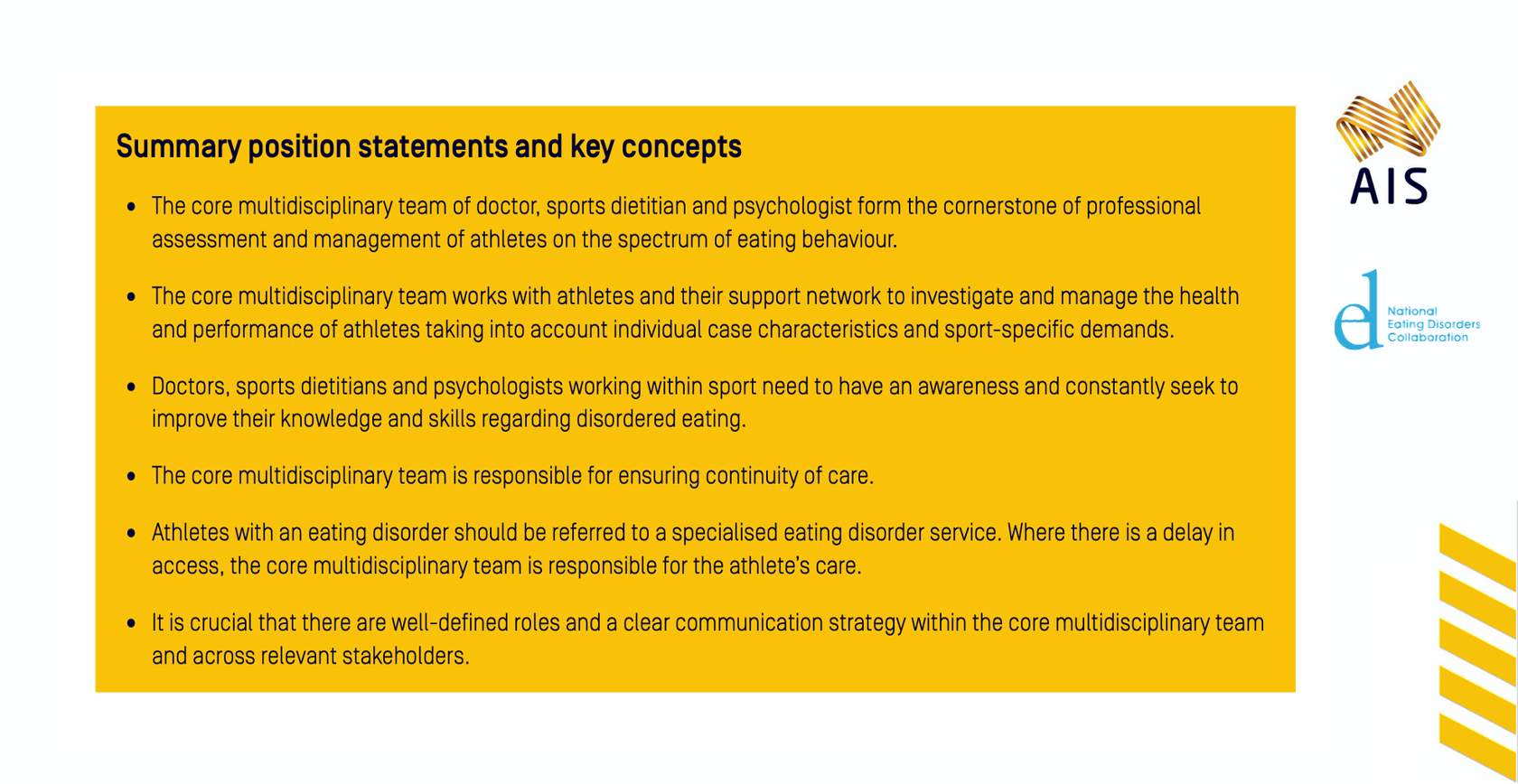
"The CMT of Doctor, Sports Dietitian and Psychologist forms the cornerstone of professional assessment and management of athletes on the spectrum of eating behaviour"
The recommended CMT is comprised of the doctor, sports dietitian and psychologist, and together they coordinate the prevention, assessment, management and maintenance care in possible DE cases. As per the Olympic Movement Medical Code, all activities of the CMT should be based on the premise that the health and welfare of athlete are pre-eminent and prevail over competitive, economic, legal or political considerations.40 Each member of the CMT provides expertise in a mutually supportive manner (see Figure 4) to deliver optimal care for the athlete in a safe, supported, individualised and purposeful way, governed by the ethos, ‘do no harm.’ Doctors, sports dietitians and psychologists working within sport, despite not always self-identifying as experts in this field, need to have an awareness of DE and EDs and regularly seek professional development in this area.
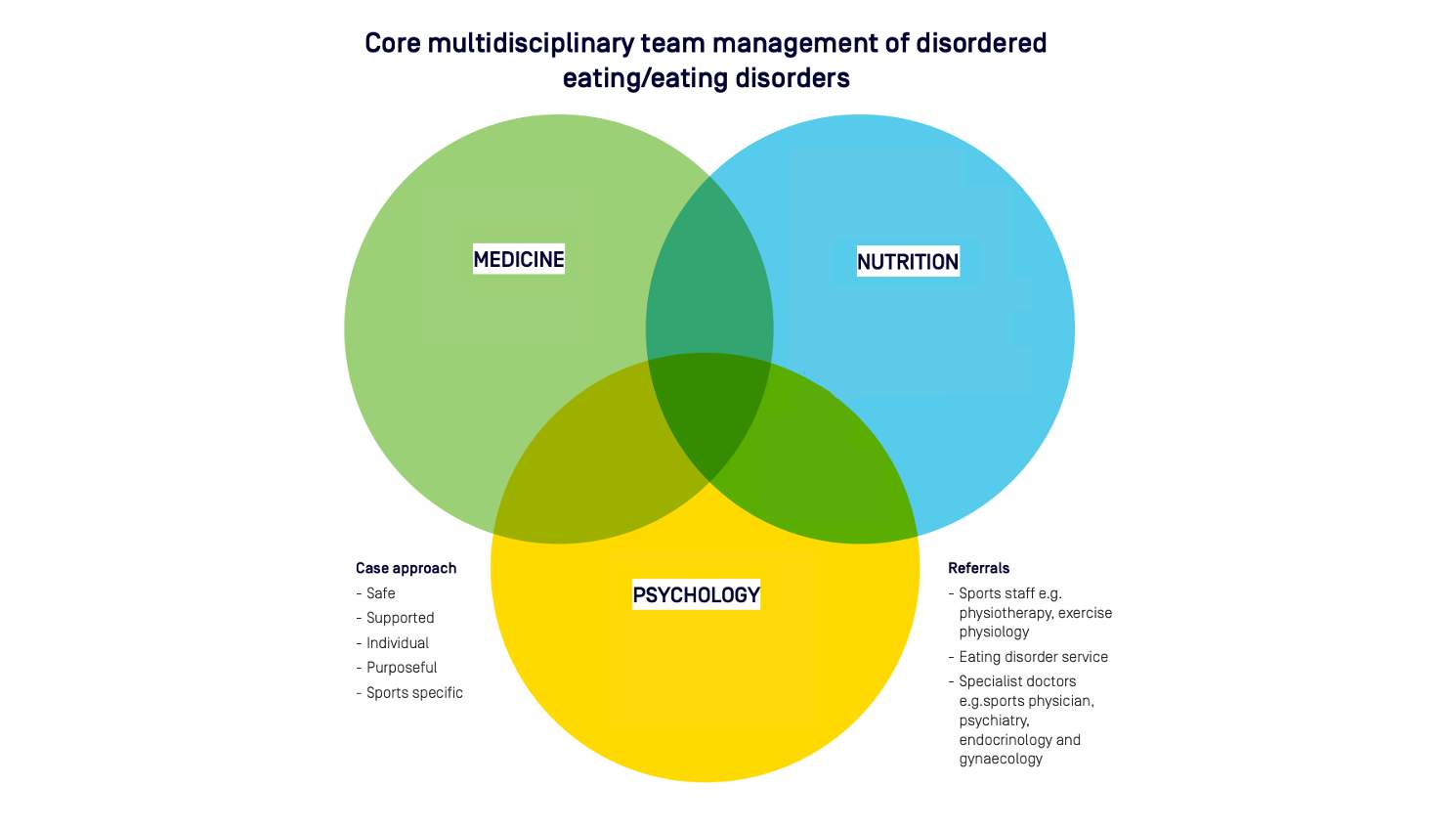
Figure 4: CMT management by a Doctor, Sports Dietitian and Psychologist: The CMT drives the assessment for DE of an athlete, which may involve some overlap between disciplines depending on the trigger for recognition of DE and the individual case characteristics.
Medicine
- History
- Examination
- Investigations
- Referrals
Nutrition
- Screening tools: questionnaire, interview
- Diet history assessment
- Special diets
- Allergies/intolerances/restrictions
- Eating behaviour
- Eating/food attitudes/beliefs
- EA assessment: RMR + DXA body composition for FFM
Psychology
- Screening tools and questionnaires
- Personality and risk factors
- Suicide risk assessment
- Protective factors
The CMT works with the athlete, coach and support staff to investigate and manage health, performance and return to play (RTP) considerations. The unique circumstances of each case are taken into account, along with sport specific demands. With the athlete’s permission and respecting patient confidentiality, the ideal management model includes regular and collaborative communication between the CMT and coach. Further input may be sought from a range of specialists including an endocrinologist, gynecologists', psychiatrist, sport scientist, physiotherapist, occupational therapist, social worker, pediatrician and/or specialist ED service (see Figure 5).14 38 Where providers are external to the sport system, the CMT plays a central role in ensuring all parties are aligned and working effectively in the best interests of the athlete. The CMT is responsible for ensuring continuity of care. This includes effective collaboration between physical and mental health services, private and public health services, sport and community-based services and between professional disciplines.
Disordered Eating Flow Chart
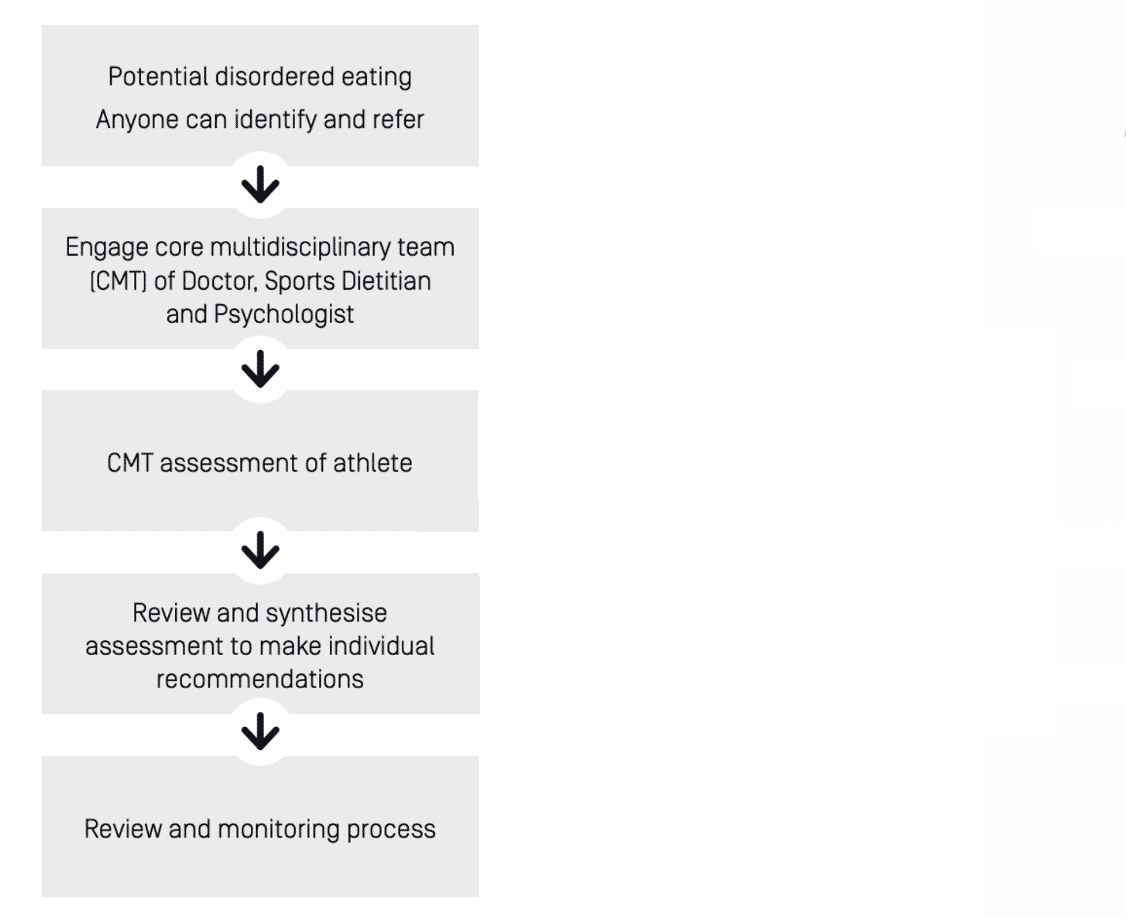
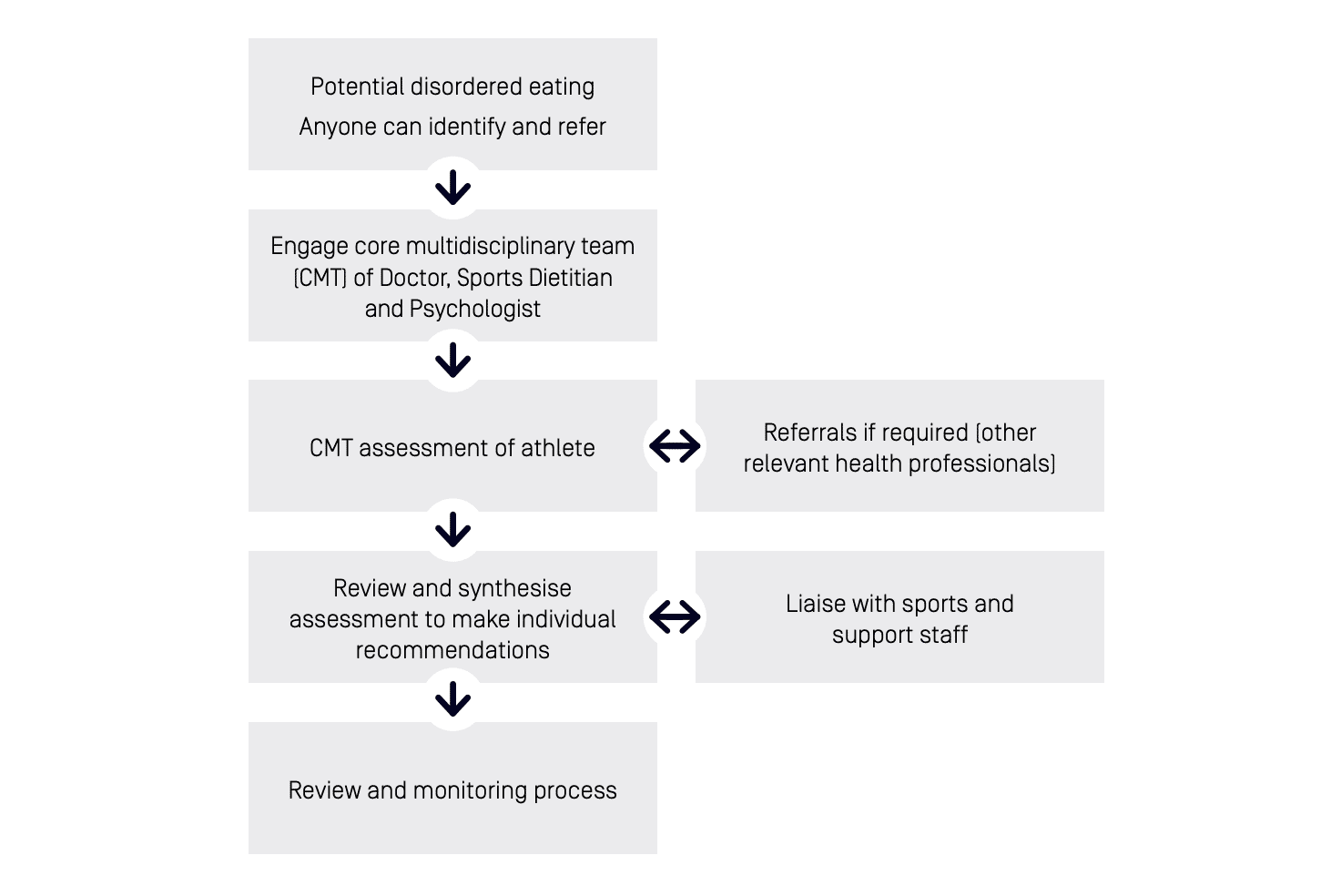
Figure 5: DE flow chart: Recognition of DE and referral of an athlete for assessment and management, primarily by the CMT within the context of a healthy sport system.
Members of the CMT may not have specialised skills in the treatment and management of EDs. Regardless, under the Core Workforce Competencies in the National Practice Standards for Eating Disorders1 , all CMT members should have the skills to be able to contribute to a comprehensive assessment and identify a clinical ED, to refer the person to appropriate service providers (in the community, intensive or inpatient settings as required), to ensure continuity of care between service providers and to provide ongoing management to a person while they are waiting for treatment. CMT members should seek professional assistance as required, through clinical supervision and/or tertiary consultation with the relevant state or territory specialist ED service. Any clinician providing treatment for an ED should do so in accordance with the appropriate clinical standards. These include the Royal Australian and New Zealand College of Psychiatrists clinical practice guidelines for the treatment of EDs (2014)2 and the UK National Institute for Health and Care Excellence guideline on EDs Recognition and Treatment (2017).3 In addition, the Australia and New Zealand Academy for Eating Disorders clinical practice and training Standards are due for publication in 2020.4-6
Early intervention should assess potential contributors and causes of DE (i.e. individual and environmental risk factors) and aim to minimise risk of developing an ED. Treatment or tertiary intervention typically focuses on addressing and reducing factors which maintain or perpetuate DE or ED, with the intention to ensure the athlete’s safe return to full sport participation. Recovery is considered to be achieved when those affected are indistinguishable from their healthy counterparts on all ED measures.41 This includes: the athlete no longer meets diagnostic or screening criteria for any ED or for DE; the athlete is no longer engaging in any DE behaviours; the athlete is in good physical health with optimised nutritional intake for levels of activity; the athlete has positive attitudes towards themselves, food, their body, their ability to express emotions and to interact socially, and; the athlete has a quality of life which includes the ability to engage in work, sport, education where relevant, and leisure.41 Regardless of where an athlete falls along the eating behaviour spectrum, the treatment goal is to shift them towards recovery, through the demonstration of healthy eating behaviour, anxiety reduction and appropriate body image.
It is crucial that there are well defined roles and a clear communication strategy within the CMT and across relevant stakeholders. A designated member of the CMT should ideally coordinate the flow of information across the team and with relevant sports staff.
Assessment of Disordered Eating in Athletes
"The combination of screening tools and clinical interviews form a foundation for DE identification in athletes"
Clinical judgement and an understanding of the high performance sport context is crucial in distinguishing acceptable from problematic behaviours. DE and dieting may be well-established in the sport culture (i.e. endorsed and/or normalized while not necessarily safe or appropriate). Unhealthy environmental cultures contribute major risk factors towards the precipitation and perpetuation of DE and EDs.
Warning signs in the general population may be masked within the sporting environment. For example, a disciplined training diet and preoccupation with body weight and shape may reflect a specific sport culture, changes in, or absolutely low, levels of body fat may be balanced by muscle to present an acceptable body weight, and excessive exercise is easily hidden by demanding training programs.42 43 Appropriate training or supervision is required to apply DSM-5 diagnostic criteria to individuals in high performance sport. A comprehensive review of ED diagnoses is outside of the scope of this position statement. Although a number of tools have been developed to screen for DE and EDs in the general population, validated and specialised tools for use in sport across varied athlete populations are limited in number and quality.33 44 45 Current recommendations for DE assessment include using self-report screening tools followed by an interview-based assessment, and sport-specific versus general approaches where available.11 13 Thus the combination of screening tools and clinical interviews form a foundation for DE identification in athletes.
Practitioner familiarity with an individual athlete facilitates the identification of relevant changes from their prior or usual behaviour. Whenever feasible, and with the athlete’s permission, assessment may involve interviewing others in the athlete’s support network, including coaches, teammates, family and friends. Seeking observations and potential concerns of others’ helps to triangulate athletes’ self-reported behaviours. The quality of the athlete support network should be assessed and decisions made regarding the requirement for education or other resources. The development of trust and a therapeutic alliance is critical during initial contact to evaluate DE behaviour. This is facilitated by active listening and well-developed interviewing skills.
Screening Tools and Questionnaires
There are a range of screening tools and questionnaires available to assist the assessment of DE in athletes. The Eating Disorder Examination (EDE) is regarded as the gold standard for clinical interview for diagnostic purposes of EDs in the general population.46 The EDE 17.0 is the newest form which reflects changes to ED classifications in the DSM-5.47 The Eating Disorder Examination Questionnaire 6.0 (EDE-Q 6.0) is a short form screening tool based on the EDE 17.0 and is acceptable for use in practice. The EDE-Q 6.0 should form part of a comprehensive assessment of the athlete. Additional tools including the Athletic Milieu Direct Questionnaire Version 2 and Physiological Screening Test, The Brief Eating Disorder in Athletes Questionnaire Version 2, and the Eating Attitudes Tes-26; all provide discrimination between athletes with and without EDs.45 48-51 However, there are several limitations of these tools for EDs, particularly for male athletes, and care should be taken to ensure the tool is appropriate for the athlete.52
The assessment of LEA in athletes is also problematic since, although the concept is robust in principle, a quantitative assessment of EA is time consuming and marred by errors of reliability and validity in calculating its main components (energy intake and exercise energy expenditure).15 The assessment of EA is complicated by errors in the measurement of its component parts and failure to account for other factors such as dietary quality and with-in day spread.15 The Low Energy Availability in Females Questionnaire is a validated screening tool which may indicate the need for more in-depth assessments such as the measurement of resting metabolic rate or hormonal status.53 However, it is noted that this questionnaire has been principally developed from endurance-trained populations and is unlikely to be as specific and sensitive in other sporting groups
In a review of measurement tools used with athletes, Pope et al. (2015) identified five measures, including the Eating Attitudes Test-26 (EAT-26), Eating Disorder Inventory-2 (EDI-2), Bulimia Test-Revised (BULIT-R), Questionnaire for Eating Disorder Diagnosis (QEDD), and the Eating Disorder Examination (EDE), none of which were developed for use with an athlete population. Though used less often in athlete research, only three measures have been specifically created for administration with athletes – the Weight Pressures in Sport Scale for Male Athletes (WPSS-A), the ATHLETE Questionnaire (AQ) and the Athletic Milieu Direct Questionnaire (AMDQ). Among these, the EAT-26 and QEDD have demonstrated validity.51 54 55
It appears that the need for athlete-targeted screening tools is even more critical in male athletes. Chapman and Woodman (2016) commented on this while performing a meta-analysis to examine whether male athletes exhibited higher levels of DE than non-athletic cohorts. They concluded that the EAT-26 was the only tool that differentiated male athletes from nonathletes and, therefore, DE assessment tools more specifically suitable for males are required.56 Male-oriented concerns about body image and eating appear to be distinctly different of those of females.57 Limitations of the current screening tools for EDs, particularly for male athletes, include the focus on drive for thinness while lacking a focus on drive for muscularity. Although clinicians may continue to use existing DE and ED screening tools, further work on athlete-focused resources should be considered a priority. Further work to increase the validity of existing DE screening tools in broader athletic populations is underway while new screening assessment tools are in the validation phase.
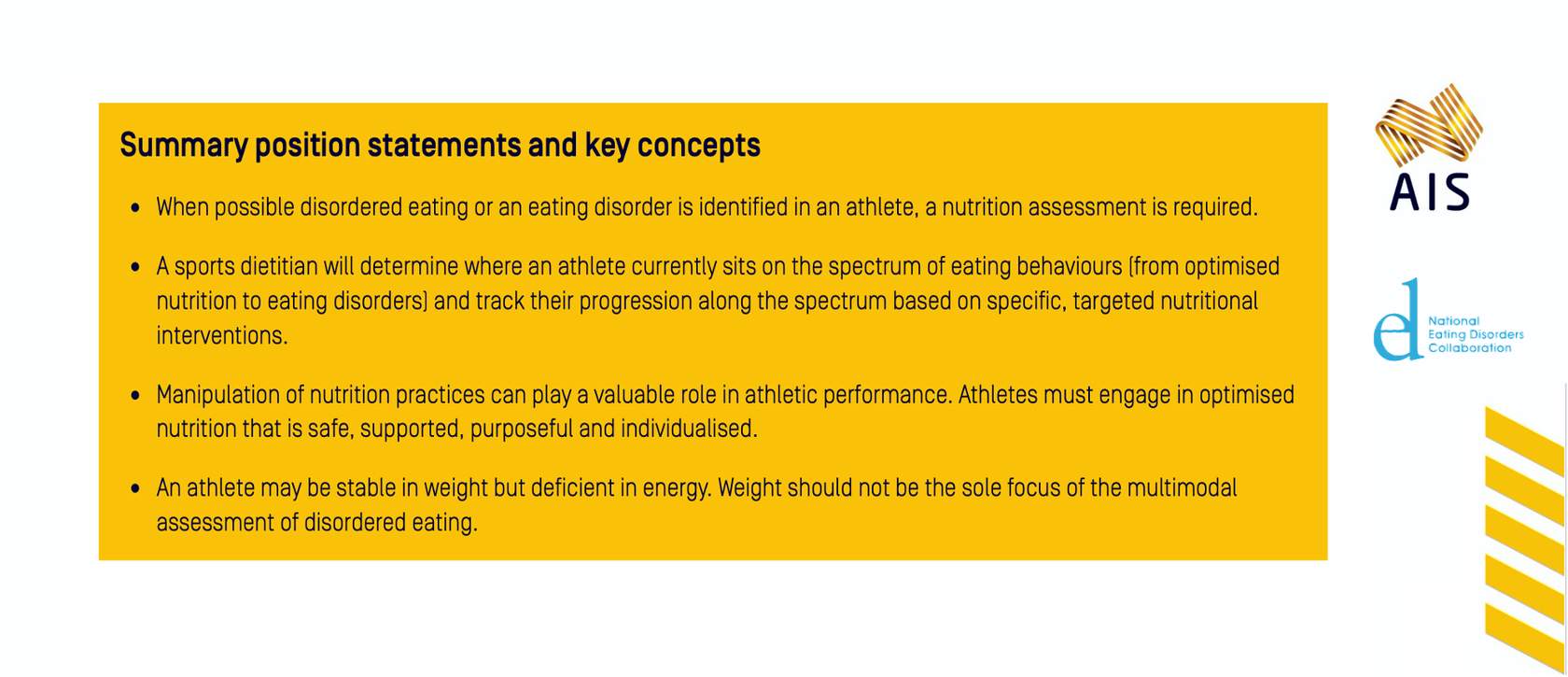
Nutrition
Nutritional Assessment
An athlete identified with possible DE should be referred to a sports dietitian for nutritional assessment of DE, EDs and LEA (See Table 5). The sports dietitian who is adequately trained in ED screening and assessment may be the first to identify concerning eating behaviours and/or thoughts and would engage the CMT to ensure a comprehensive assessment of the athlete is completed. The sports dietitian can conduct screening questionnaires and interviews; complete a diet history and nutritional assessment; assess for the presence of special diets and restrictions/intolerances/allergies; perform an EA assessment; evaluate risk factors and warning signs of DE or EDs and assess where an athlete is on the spectrum of eating behaviour (see Figure 1). An athlete may be stable in weight but deficient in energy. Weight should not be the sole focus of the multimodal assessment of DE. The sports dietitian aims to understand the psychological component to food choices; the athlete’s views of their body and how these thoughts may impact on food selection. In some cultures and countries, food security may overlay food choice and eating behaviours. A sports dietitian will look to challenge and monitor the athlete’s capacity to move along the spectrum. This is an important component of initial and ongoing nutrition assessments in both the presence and absence of an ED. Tracking where an athlete sits on the spectrum of eating behaviour helps a sports dietitian to better understand the athlete and apply appropriate and targeted nutrition interventions. An athlete’s ability or inability to follow nutrition advice/recommendations also provides further information as to where the athlete sits on the spectrum.
Table 5: A nutrition assessment of the athlete with possible DE includes information on a range of issues.
Behavioural
- Current eating patterns
- Eating behaviour history
- Special diets followed, particularly if the diet involves avoidance of certain foods and/or if the range of foods to be avoided has increased over time
- Specific food restrictions in place, whether for medical or for personal reasons
- Food rules and beliefs
- Flexibility or rigidity around food or nutrient intake
- Current and past nutritional supplement use
- Social interaction with food and meals (any isolation or withdrawing)
- Compensatory behaviours (e.g. vomiting, laxative use, diet pills etc)
Physical
- Pathogenic weight control practices
- Adequacy of current dietary intake including overall energy, macro- and micro-nutrients
- Current and past history of weight and body composition (are these stable or do they fluctuate)
- Active pursuit of changes in body composition, including the time-course and methods of achieving these changes
- Training load and phase
Medical
- Review of biochemistry
- Food allergies and intolerances
- Menstrual history, current menstrual pattern
- Medication (including combined oral contraceptive pill)
- Gastrointestinal complications
- Family history of dieting, eating disorders, mental health issues, relationship with food
- EA assessment (with various methods including RMR and DXA body composition for FFM)
Emotional
- Food and eating attitudes
- Current and past relationship with food and body
- Amount of time spent thinking about food, weight and body image
- Body image, past and present (considering both athlete and general population body image)
Nutrition for health and performance
Manipulation of nutrition practices, including the short-term implementation of special dietary strategies around competition periods, plays a valuable role in helping athletes to achieve their performance goals. Nevertheless, nutrition for athletes needs to encompass considerations of both health and performance, often needing to find a balance between opposing practices or goals. The characteristics of optimised nutrition in an athlete include:
- They are able to meet their physical and mental health needs via their eating practices
- They are able to adapt their intake to meet the specific and changing demands of their sport,
- They have flexibility around their eating and thoughts about food,
- They are able to eat socially
- They are free of restrictive behaviours such as the avoidance of whole food groups; excessive counting of calories or macro nutrients; or rigidity around foods consumed,
- They have a healthy body image.
A plan for optimised nutrition should be safe, supported, purposeful and individualised as illustrated by Figure 6. Nutrition practices are considered safe if they support the principle of ‘at first do no harm’ and in doing so, fundamentally prioritise athlete physical and mental health. The delivery of these optimal practices is supported when guided by the appropriately qualified and experienced members of the CMT with interaction and input from the wider performance team.

Medicine
Medical Assessment
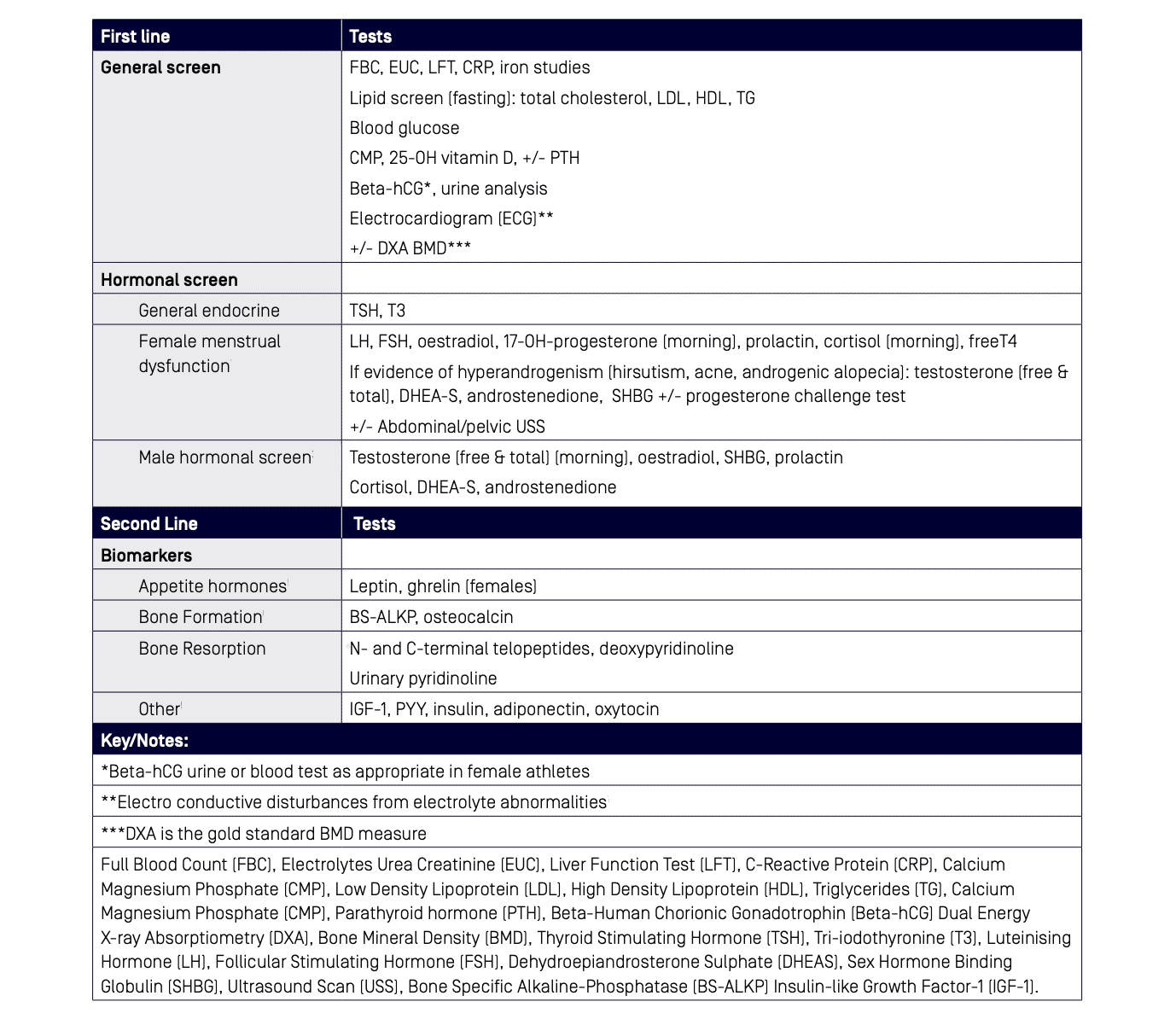
The medical assessment of an athlete with identified DE should include thorough history (Table 6), examination (Table 7) and investigations (Table 8) based on information provided by the athlete and CMT. All athletes with bone stress injury and/or menstrual dysfunction should be screened for LEA/RED-S and screened/assessed for DE and EDs. Care should be taken to select appropriate first-line and second-line investigations for the individual case to complete general and hormonal screenings, bearing in mind the timing of testing as it may relate to diurnal fluctuations, fasting status and menstrual cycle if known. Second line biomarkers (Table 8) of appetite, bone formation/resorption and other potential LEA indicators are an evolving space with some markers, such as ghrelin, currently only used in research settings. Consultation with an endocrinologist for interpretation of results may be required if outside the expertise of the practitioner. Referral to an appropriate specialist should be considered for more complex cases with valuable contributions frequently obtained in the fields of endocrinology, gynaecology and psychiatry.
Table 6: Medical history when assessing an athlete with DE.
General
- Medical
- Surgical
- Musculoskeletal
- Family history (ED, osteoporosis (OP), menstrual)
- Medications and supplements
- Allergies
Bone Health
- Bone stress injury
- BMD
- Calcium intake
- Vitamin D (sunlight & dietary intake)
- Mechanical loading
- Family history OP
Female
- Age of menarche
- Length and frequency of periods (number of cycles per year), regularity, last normal menstrual period, flow
- Amenorrhoea (frequency and duration)
- Oral contraceptive use
Male
- Loss of morning erections
- Decreased libido
Table 7: Examinations to perform when assessing athletes with DE.
Basic Observations
Heart rate (HR), Blood Pressure (BP), (including postural measures of HR and BP) temperature
Pre-Participation System Examination
Cardiorespiratory, abdominal, thyroid, ear/nose/throat, lymph nodes
Specific Systems of Concern
Bone stress injury examination
Advanced ED
Lanugo, particularly, sub-conjunctival haemorrhages, swelling of parotid glands, erosion of tooth enamel, bradycardia, peripheral oedema
Primary Amenorrhoea
Gynaecological examination recommended
Adolescent
Stage of sexual maturation (Tanner)
Table 8: Investigations to perform on athletes with suspected DE
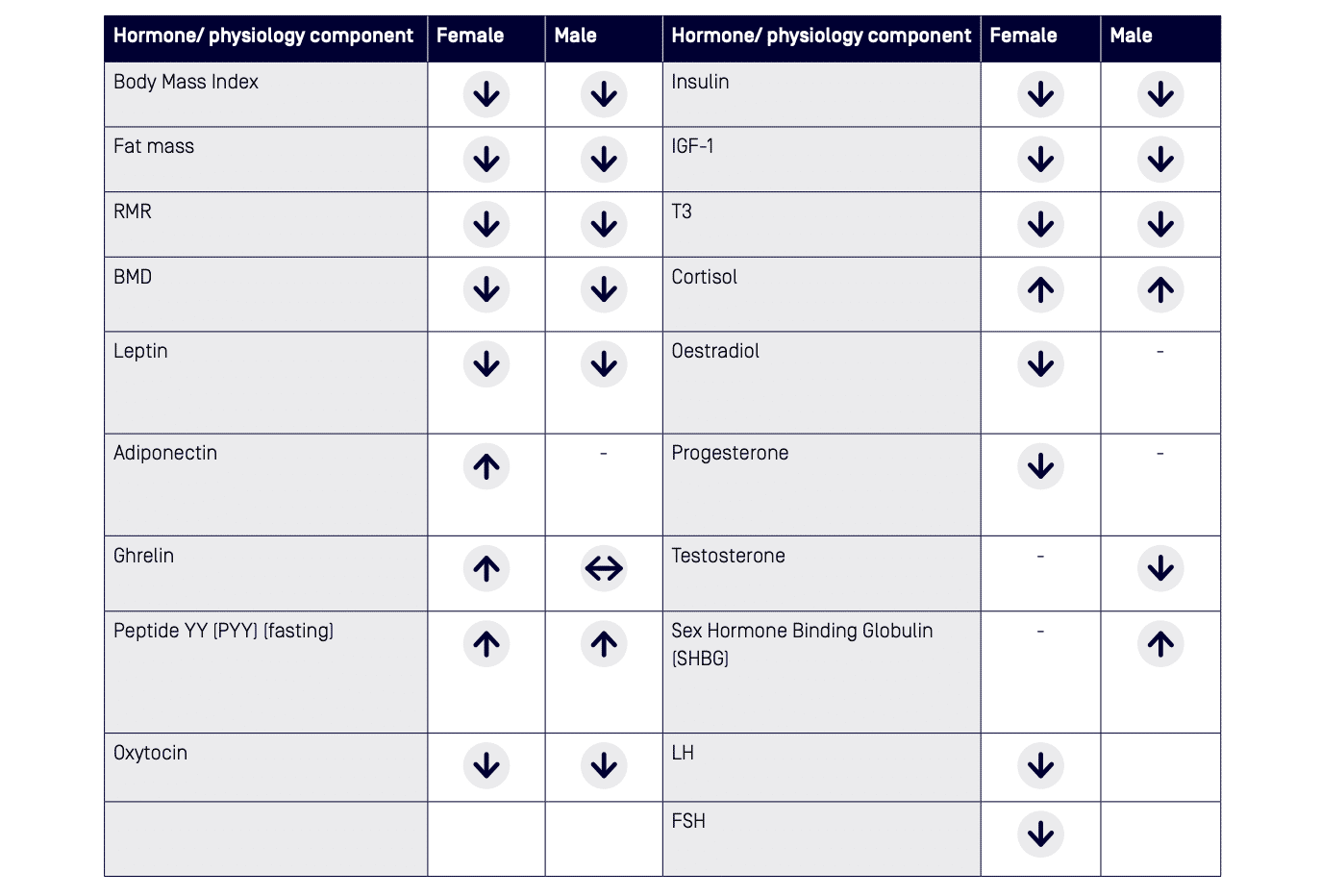
A summary of the endocrine effects of RED-S by Elliott-Sale et al. (2018) provides the latest background on hormonal/ physiological profiles in LEA in men and women which has been combined with other data to create Table 9.28 53 62 While some biomarkers/hormones show significant change in female athletes, menstrual dysfunction may be a more readily detectable clinical sign of LEA. 19 Importantly, menstrual dysfunction should not be accepted as an inevitable consequence of being an athlete and should be investigated. Furthermore, hormonal profiling in a female taking hormonal contraception is not clinically useful. Hormonal profiling may be considered after a trial of three months off the combined oral contraceptive pill (COCP). Changes in biomarkers/hormones in males are different from those in females and may occur at a lower EA cut-off.24 The long-term consequences of impaired hormonal health in male athletes is not well established and requires further research.
Table 9: A summary of the potential hormonal and physiological changes in athletes with LEA synthesised from the articles; Parallels with the female athlete triad in male athletes by Tenforde et al. (2016), Low energy availability in athletes: A review of prevalence, dietary patterns, physiological health, and sports performance by Logue et al. (2017), Endocrine effects of RED-S by Elliott-Sale et al. (2018.)
Bone Health
Optimisation of bone health is important for short-term and long-term health and performance outcomes and involves the attainment of peak bone mass (between 18 year and 22 years of age) and prevention of accelerated BMD loss thereafter. 7 16 63 A medical workup of an athlete with any combination of DE or ED, bone stress injury, menstrual and/or hormonal dysfunction should take into account various modifiers of bone health (see Table 10). Instigation of appropriate pharmacological and bone loading treatment may be required. An athlete involved in non-weight bearing and/or endurance sport (eg, swimming or cycling) should consider a programme involving drop jumps to satiate ground reaction force contribution to bone health64 65, a typical programme might involve a two-footed landing from a 30cm platform, repeated 10 times with 10 second gap between jumps.
Table 10: Bone health modifiers
Nutrition
- Recommended dietary intake of calcium, vitamin D and optimal energy availability
- Adequacy of general diet (e.g. protein)
Environment
Sunlight exposure and vitamin D status
Sport Specific Mechanical Loading
Weight-bearing and other bone loading activities
Medical History
Existence of co-morbidities affecting bone metabolism (e.g. diabetes, pituitary, renal or gastrointestinal disease)
Hormonal
Hormonal influences (low oestrogen and/or testosterone)
Iatrogenic
Medications affecting bone (e.g. oestrogen, progesterone, glucocorticoids and anabolic steroids)
Athletes with six months or more of LEA, DE, ED or amenorrhoea should have BMD measured by dual energy X-ray absorptiometry (DXA),16 as per the guidelines of the International Society of Clinical Densitometry (ISCD) and the American College of Sports Medicine . 62 67 Assessments should refer to Z-scores (age-matched and sex-matched). In the athletic population, low BMD is defined as a Z-score between -1 and -2 standard deviation (SD), together with a history of nutritional deficiencies, hypo-oestrogenism, stress fracture or other secondary clinical risk factors for fracture. 16 As athletes in weight bearing sports should have a BMD that is 5-15% higher than non-athletes, a BMD Z-score less than -1 SD warrants further attention. 16 DXA assessments should be repeated in at-risk adults every 12 months and in at-risk adolescents at a minimum of every six months, preferably using the same DXA machine.16
Calcium supplementation may be required if the recommended daily intake is not met from food sources but such decisions should be made only after a thorough dietary assessment by a sports dietitian. Guidelines for calcium intake vary slightly between countries with the daily recommended dietary intake of calcium 1000 mg for men and women aged 19-50 years in Australia and the USA, and 1300 mg for children and adolescents, aged 12 – 18 years in Australia, and 9 – 18 years, in the USA.68 69 While the biochemical cut-off for vitamin D deficiency is controversial70-72, blood levels <50 nmol/L in winter months or <75 nmol/L in summer months should be considered for supplementation.70 The endocrine society clinical practice guidelines provide current recommendations for vitamin D supplementation across age ranges and subpopulations.73 Vitamin D deficient adults can be treated with 50 000 IU of vitamin D once a week for 8 weeks, followed by maintenance therapy of 1500-2000 IU daily, with repeat serum vitamin D testing to assess response and prevent toxicity.73 Inadequate EA is likely to be the most important dietary cause of poor bone health; there is evidence of suppressed bone formation once EA decreases below 30 kcal/kg FFM/day in women62 while impaired bone health is likely to occur below 20-25 kcal/kg FFM/day in men. 24 74 LEA suppresses bone formation and low oestrogen contributes to upregulation of bone resorption.62 Annual BMD losses in amenorrhoeic, oligoamenorrhoeic or menopausal women can increase from 0.3% as seen in eumenorrhoeic women, to 2% per year.75 Serum testosterone within the lowest quartile of the normal clinical range (total testosterone 9-38 nmol/L) is associated with an increased risk of bone injuries in males
Females Athletes
Table 11: Definitions of menstrual function in female athletes.
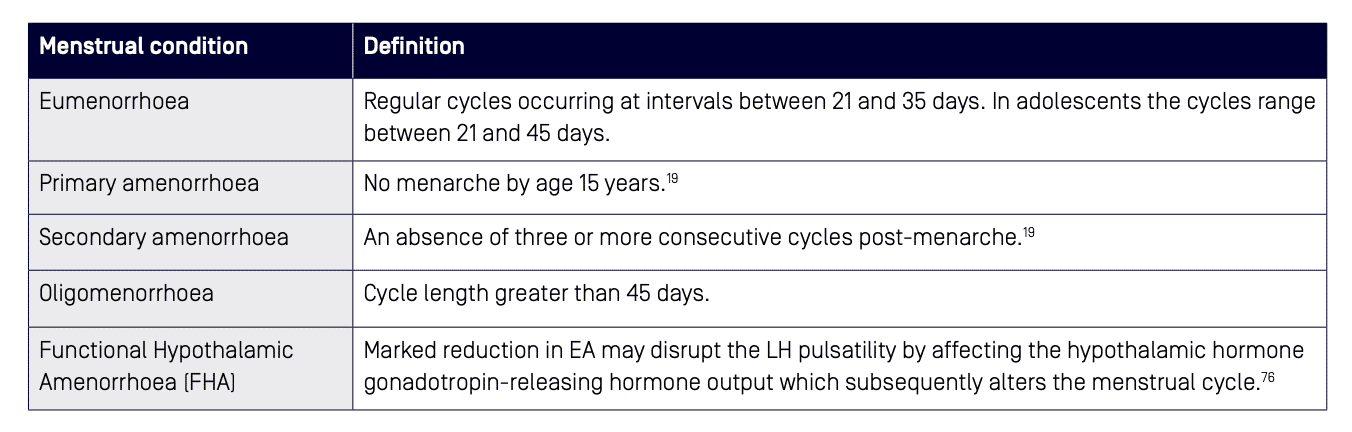
Table 11 summarises various terms used to describe the menstrual function of females. Amenorrhoea may occur in up to 66% of athletes77, but its presence for more than three months should not be accepted as an inevitable consequence of being an athlete and must be investigated.13 Aetiology of oligo-amenorrhoea may include pregnancy, primary ovarian insufficiency, hyperprolactinaemia, thyroid dysfunction, polycystic ovarian syndrome (PCOS) and functional hypothalamic amenorrhoea (FHA), which is a diagnosis of exclusion.16 61 The underlying cause of FHA is LEA rather than exercise volume or body composition, thus optimisation of EA should be the first line treatment of FHA28, however it may take more than six months for favourable menstrual changes.62 Assessment of an athlete with menstrual dysfunction by a sports dietitian forms a part of the complete care of the female athlete.
The triad amenorrhoea algorithm (Figure 6) provides a succinct and systematic approach to diagnosis and referral of an athlete with menstrual dysfunction.60 The clinical signs and symptoms of menstrual dysfunction can be used as a surrogate marker for LEA, but these may be masked by concurrent use of oral contraception. Treatment of menstrual dysfunction via supplementation with exogenous hormones, such as the COCP, does not correct the cause of FHA and does not protect against BMD loss.7 16 28 61 To protect BMD in these athletes, it is preferable to use transdermal oestrogen, with cyclic oral progestin as an adjunct16; this is applied twice weekly as a transdermal 17Beta-oestradiol (E2) patch (100 µg), with cyclic micronised progesterone (200 mg) for 12 days each month.61 The transdermal hormones are not a form of contraception and risk factors which may preclude use of the COCP should be considered
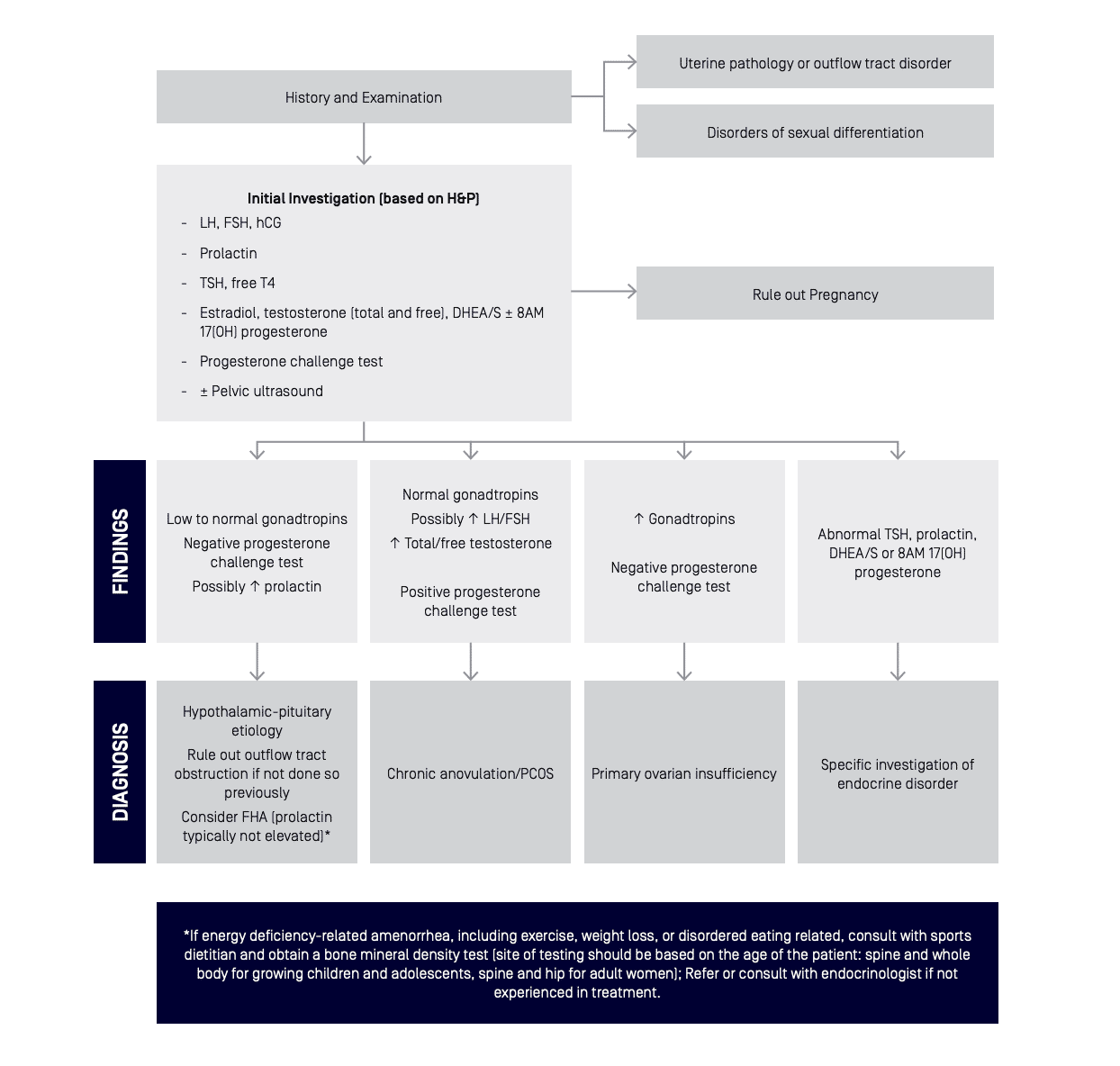
Figure 7: “Amenorrhoea algorithm. Recommended clinical evaluation of an athlete with primary or secondary amenorrhoea, or prolonged oligomenorrhoea, includes a history and physical examination, initial and followup laboratory testing, and diagnosis by a physician. Referral or consult with endocrinology is recommended if the diagnosing physician is not experienced with treatment of FHA or other aetiologies of amenorrhoea. LH, luteinising hormone; FSH, follicle stimulating hormone; hCG, human chorionic gonadotropin; TSH, thyroidstimulating hormone; DHEA/S, dehydroepiandrosterone sulphate; FHA, functional hypothalamic amenorrhoea; PCOS, polycystic ovarian syndrome. Modified from Illingworth.”
Male Athletes
LEA may suppress reproductive and metabolic hormones in men at <20-25 kcal/kg/FFM/day11 but the clinical signs and symptoms are relatively subtle.28 53 62 Reduction in libido and loss of nocturnal penile tumescence may be a sign of relative reduction in testosterone. A relative reduction in testosterone that may remain at a subclinical threshold may be seen in the LEA state.24 Testosterone is best measured as a fasted, morning sample to avoid wider fluctuations throughout the day. A serial/longitudinal record for the individual in the clinical context may be more beneficial than a single measurement.28 A study of male endurance athletes by Heikura et al. (2017) showed that those with the lowest quartile of testosterone within the normal range (total testosterone 9-38nmol/L), were more likely to self-report food patterns consistent with LEA, while having lower T3, and 4.5 fold higher rates of bone injury than the rest of their cohort.
Psychology
Psychological Assessment
Mental Health
A comprehensive mental health evaluation is critical to determining intervention and treatment, and can be provided within the CMT by a psychologist or doctor with mental health training.79 A mental health evaluation aims to determine range and severity of DE symptoms, diagnose EDs and other mental illnesses, and identify any immediate medical or psychological risks. Co-morbidity of mental illness is high across ED categories, with mood disorders, anxiety disorders, alcohol and other substance use, and personality disorders as the most common.80 EDs have one of the highest mortality rates of all psychiatric illnesses, and those diagnosed with an ED have significantly elevated suicide risk.81 82 83 Therefore a suicide risk assessment should be undertaken alongside any assessment where DE or ED may be indicated. Risk assessment should include current and prior history of suicidal ideation, self-harm and self-injury, suicidal behaviour, agitation and risk of harm to others.
The use of interview protocols is well suited to evaluating eating behaviours and beliefs according to DSM-5 diagnostic criteria. This is best achieved through casual conversation using a semi-structured protocol, which allows for follow-up questioning where indicated. The EDE 17.0 or EDE-Q 6.0 can be used for these purposes, as can a general mental health evaluation such as the Mini International Neuropsychiatric Interview (MINI 7.0.2).84 The MINI 7.0.2 provides a diagnosis of prior and current comorbid conditions, including EDs as well as suicidality. When a focussed ED or comprehensive mental health evaluation is required, this should be done by an appropriately trained mental health provider.
Readiness for Change
Where DE symptoms are detected or there is a high risk of developing an ED, additional information regarding the athlete’s readiness for early intervention and treatment is important. This includes the athlete’s readiness to change, anticipated challenges as well as strengths or protective factors. The athlete’s readiness to change, or motivation for treatment is a consistent predictor of treatment success.85 Change does not occur in a linear step-by-step manner but rather reflects a dynamic process. An athlete may not be considering change at all, perhaps unaware or in denial (pre-contemplation), may be considering change but not taken any action (contemplation), giving more serious thought to change in preparation to initiating early attempts (planning, action), or may be sustaining change and proactively preventing and coping with relapses (maintenance). Behaviour change made early has predicted better outcomes in both AN and BED86, underscoring the importance of early identification and effective management. Motivation to change among athletes with DE fluctuates often during treatment, and regular assessment can guide the broader support network to promote and strengthen athletes’ readiness to change.
Personality
Elite athletes commonly exhibit psychological traits associated with DE which also enable successful performance, such as high achievement orientation, self-motivation, self-discipline and perfectionism.13 Personality has long been linked to the onset and maintenance of DE. 88 89 For example, AN or restricting behaviours are commonly associated with higher levels of constraint and persistence, where binge-compensatory behaviours are linked to impulsivity when emotionally distressed.88 While some personality traits separate different ED types, other traits are common across most people diagnosed with an ED (NEDA Toolkit – Temperament and personality).90 Women with AN and BN were found to be more likely than healthy controls to have exhibited signs in childhood of obsessive-compulsive personality traits (perfectionism, inflexibility, rule-driven, drive for order and symmetry, excessive doubt and cautiousness), and the presence of one or more of the traits increased one’s odds from seven to thirty-five times more likely to develop an ED.91 In addition to obsessive-compulsiveness, high degrees of perfectionism have been reported among those with AN and BN.92 93 While personality and ED behaviour are clearly linked, sustained starvation/LEA bring about changes to thoughts and behaviour that make it difficult to separate causes from consequences.
Family and Social Networks
In addition to mental health, psychologists will also examine the athlete’s psychosocial history, social support and perceived stress across relevant life domains (sport, school/work, social). Family history of mental illness is also relevant, particularly the presence of DE or body image disturbances. This may suggest genetic risk but also indicates where the family may be reluctant to address problematic perceptions and eating behaviour, or inadvertently act in ways that trigger or maintain DE behaviour.
As part of the social network, assessment and engagement of parental support early in the process is important to facilitate implementation of the recommended intervention, particularly if health deteriorates.13 In high performance sport, instances arise where the heavy parental involvement in the sporting success of the athlete causes difficulty in accepting that there is an issue with DE. Members of both the sport and personal network can be adversely impacted by athlete’s DE or ED and should be actively and appropriately engaged as part of treatment given, they are important allies. Depending on the age and autonomy of the athlete, parents and guardians may have some responsibility in the management and treatment. A well-established support network that is well aligned and trusted can be protective factor, however it is also imperative that important others are adequately prepared, ready and resourced to have this role in order to minimise undermining the athlete’s or CMT efforts.
The complexity of DE requires a biopsychosocial approach, and it is important to know the type and nature of support within the athlete’s social network. An evaluation of this can be done indirectly and informally, or in a more formal manner (social network analysis) through asking who they interact with frequently, who are they most influenced by, how well they trust those individuals, and whether these interactions are distressing or harmonious. A supportive and well-aligned network is essential to successful treatment.
Treatment and Ongoing Monitoring of the Athlete with Disordered Eating
"An athlete with DE can continue to participate in sports, provided that they engage appropriately and consistently with their support team"
Once DE is identified in the high performance athlete, the review and maintenance process of care requires information sharing and progression of treatment goals between the athlete, CMT, sports coaches and support staff. A designated member of the CMT should ideally coordinate the flow of information within the team to formulate individual athlete treatment and maintenance goals, clearly outlining medical and behavioural objectives to ensure safety and sports-specific RTP criteria. This requires engagement with the athlete and follow through from sports staff. A large amount of information is typically collected in areas of nutrition, medicine and psychology; a consistent, systematic approach is required to ensure that all avenues have been explored and openly communicated. The CMT can formulate a timeline for maintenance and review.
Modifications, Exclusions and Return to Play Decisions
Modifications to an athlete’s training within the context of DE is complex. Given the potential for injury and/or illness if an athlete continues to train through DE, there may be times when training modification or full exclusion is required. An ED diagnosis may not be needed to justify the need for modification to training and/or competition to ensure the athlete’s safety.
RTP decisions should be made by the CMT in collaboration with the coach(es) on an individual basis, taking case characteristics and sport specific demands into account. It is reasonable that athletes with DE can continue to participate in sports, provided they engage appropriately and consistently with their support team. Each sport governing organisation or federation should have guidelines to support difficult decisions with respect to affected athletes and the particular diagnoses (e.g. RED-S).
Clinical assessment tools which may assist and guide decision making in relation to RTP, include the RED-S Clinical Assessment Tool and the 2014 Female Athlete Triad Coalition Consensus Statement (female athletes with DE, menstrual dysfunction and low BMD). Currently, there are no accepted values for sport-specific minimum or optimal levels of body fat or body weight. As such, these values should not be set by sporting organisations. Within the clinical ED treatment environment, the Safe Exercise at Every Stage guideline (SEES), may be used to guide clinical reviews and RTP plans. Athletes with an ED should be referred to an appropriate ED service and assisted to transition back into the high performance sporting environment as part of their recovery.
Prevention and Education
An environment and culture that assists in the prevention of disordered eating is of utmost importance to promoting the health of all athletes
Creating and embedding an environment and culture that assists in the prevention of DE is of utmost importance to promoting the health of all athletes and minimising DE risk and incidence. Key points of prevention identified by Sundgot-Borgen and Torstveit (2010) are to advocate health and well-being, de-emphasise body weight, use role models with diverse body weight and shape, reinforce sensible body composition, educate athletes about ‘the 24-hour athlete’, refer athletes at risk for DE, dispel the myths that ‘thinner is better’ and that ‘amenorrhoea as a normal sign of training’ and make DE a ‘health and safety issue’ not a ‘coaching issue’.31 Prevention of DE can also involve advocacy for changes to unhealthy sport rules and identifying strategies to mitigate existing ‘at risk’ rules.
Education programs are the best method of primary prevention of DE and EDs.97 The main aims of education are to reduce stigma, promote healthy relationships with food and body, encourage open and honest discussion, educate about potential health and performance consequences and educate about optimal nutritional strategies.13 Bar et al. (2016) reviewed the existing literature on ED prevention programs in athletes and found that selective, primary interventions with multiple targets (e.g. athletes and coaches) and an interactive multimodal approach are most effective at ED prevention.98 Martinsen et al. (2014) studied prevention of EDs and associated symptoms in Norwegian elite sport high schools with a randomised controlled trial and found that their yearlong intervention program prevented new cases of EDs and symptoms associated with EDs in adolescent female elite athletes compared to controls.99 The education sessions targeted not only athletes but coaches and sport administration as well. Best practice in this area would see coaches, sport support staff members and judges undergoing an initial comprehensive education program and regular refresher education sessions. Ideally a stepped care model targeting the level of education required for each roles derived from the core competencies of the NEDC National Practice Standards for Eating Disorders, 2018.1
Athlete prevention efforts are best directed at modifiable risk factors such as body dissatisfaction and low self-esteem and seek to minimise potential adverse effects of body manipulation. Three programs have demonstrated true prevention effects with EDs (i.e., Student Bodies, the Body Project, and a Healthy Weight Intervention), and media and literacy campaigns exist.100 Although none of these were developed for, or targeted specifically to athletes, they may provide useful references for designing programs which consider the unique culture of the sport environment and athlete-specific needs and values, to reflect essential components of evidence-informed practice.
Body Composition Assessment
Assessment and Manipulation of Body Composition
'Dieting’, the deliberate restriction of calories and/or specific nutrients for actions to promote the purpose of loss of body mass and/or body fat, is well documented as one of the major risk factors for developing an ED.101 Yet, physique assessment is a common activity undertaken within athlete monitoring protocols, and manipulation of body composition, including weight or body fat loss, is a common goal within an athlete’s sports nutrition plan. It is neither realistic nor necessary to suggest that these activities should be removed from the athlete’s routine in fear of causing DE in athletes without an ED history; however, the effects of the protocols, environment and context in which they are conducted should be considered to ensure that they are safe, include a prevention focus to minimise the risk of DE developing. This includes avoiding weighing and body composition assessment practices that increase risk. Studies which have examined these issues have found negative effects of self-weighing on male and female non-athletes102 as well as female athletes.103 ‘Team weigh-ins’ in military male and female populations have been found to increase pathological weight loss behaviours around times of body measurement and fitness testing, which may decrease health and performance.104 105 Indeed, in 2001 the Canadian Academy of Sport Medicine adopted a position that routine body composition assessment be abandoned for all female athletes and dancers.106
Routine assessment of body composition requires careful deliberation of the rationale for the assessment (i.e. is it purposeful and necessary), who is undertaking the measurements, the level of training required to take the measurements as well as the level of support available to the athlete to interpret the information and provide recommendations. Examples of body composition assessment techniques include (but are not limited to) body mass weighing, skinfolds and DXA. Within the Australian context, a sports dietitian who is a qualified anthropometrist is the appropriate expert, highlighting the importance of this position within an athlete’s CMT. A sports dietitian can formulate advice as to whether to test athletes or not, based on some of the following factors: history of DE or EDs, age, level of nutrition support in the domestic training environment, and the type of protocols used (weighing, skinfolds and DXA). It should be considered that the coach is not primarily involved in the body composition assessment process. The underpinning philosophies of body composition monitoring are that no harm should be done to the athlete being tested and that the data collected from such protocols should be treated as personal and confidential medical information. 107 Education regarding body composition and testing including procedure, rationale, consent and use of information must be conducted for all athletes prior to commencing any testing. All athletes should complete a consent process for body composition assessments, with parental consent where appropriate. Best practice should also ensure that expert nutrition support from a sports dietitian is provided from end-to-end: that is, from pre-assessment through assessment to advice and ongoing monitoring if manipulation of body composition is indicated.
Strategies for Safe Weighing and Body Composition Assessment
Strategies for weighing an athlete in a way that reduces anxiety about weight may be drawn from ‘trauma informed care’ practices used within ED services, with principles of choice, collaboration, trustworthiness, safety and empowerment. These include gaining explicit consent for every measurement (verbal), checking in with the athlete prior to the measurement and offering to ‘blind weigh’ the athlete so that they do not see the results of the examination.108
Protocols for this include:
- Allow the athlete to step onto the scales backwards, or otherwise obscure their view of the scales
- Refrain from discussing the athlete’s weight while they are on the scale, or use any other vocal cues which may lead them to make any inferences about their weight (e.g. “You’ve done well this week”),
- Finish the physical examination before discussing the athlete’s weight and general progress
- Withhold the specific anthropometric/numerical details of the athlete’s weight
- Provide appropriate individual privacy for weighing and confidential discussion of results
If there is any distress about being weighed or measured, this needs to be taken seriously and the coach and CMT need to discuss the appropriate course of action for this athlete.
There are some ED treatment modalities which include viewed weighing as a form of exposure therapy and monitoring (e.g. enhanced cognitive behaviour therapy),109 however these should not be undertaken by anyone who has not been appropriately trained or does not have adequate support from the CMT and clinical supervision.
A sound general principle for minimising anxiety associated with weighing is to reach an agreement as to which one member of the CMT will be responsible for ongoing monitoring of this metric, so that the athlete is not weighed or measured either too frequently, or by different clinicians and can foster trust and appropriate interpretation of results to promote continuity of care.
Body Image
Positive body image is one of the protective factors against development of EDs, and forms a foundation for most effective ED prevention programs in athletes.110 It is notable to acknowledge that negative and positive body image are two different yet intersecting constructs which both need to be taken into consideration within both the general and athlete populations.111 Petrie and Greenleaf’s theoretical model suggests that body image dissatisfaction can be a moderator of EDs amongst athletes.112 113 An athlete’s perception of their physical self, and the thoughts and feelings that are entailed, can produce perceptual, affective, cognitive and behavioural manifestations. An athlete may frequently have separate body images; an athletic body image and a social body image.112 114-116 There may be tensions between the socially desirable body image and the ideal physique for performance in the athlete’s sport.117 This can be intensified if the athlete receives attention from one source in comparison to another (e.g. attention to their sporting success is highlighted in social media; or their presence on social media becomes an issue within athletic circles). This is further complicated by potential sponsorship opportunities being tied, whether in perception or reality, to body image. Both male and female athletes may have a body image that is in conflict with cultural norms and gender stereotypes (i.e. males should look muscular and lean and females should be light and thin). Body image dissatisfaction in male and female athletes is a risk factor for DE or an ED irrespective of the perceived weight-related performance pressures of their sport.104 112 117 Some sub populations are at additional risk for body image dissatisfaction; for example para-athletes and those with concurrent conditions such as diabetes mellitus118 119 or polycystic ovarian syndrome.120 The biological changes that occur during puberty and adolescence may contrast with the ideal physique in a sport, making this a higher risk time for the development of DE or an ED.

Creating a Healthy Sport System
"Sports have a responsibility to all athletes across the entire high performance pathway to create a healthy sport system"
Support systems for healthy participation in sport involving individuals with specific expertise in DE and ED will decrease the likelihood that such problems will occur in athletes. Every sporting organisation should be aware of the increased prevalence of DE in high performance athletes and have established guidelines for early identification and prevention of DE. Guidelines should reflect this position statement, be sport specific, and promote nutrition practices that are safe, supported, purposeful and individualised. Sporting organisations need communication protocols to refer athletes to a member of the CMT, as part of accepted and routine care to support athlete health and performance optimisation. Some sporting organisations may not currently have access to a member of the CMT. Sports are strongly encouraged to build their healthcare network to ensure they engage with all roles comprising the CMT.
The rules and regulations for specific sports can influence prevalence of DE behaviours in athletes.121 Sport specific changes in rules and regulations may assist in reducing the prevalence of DE behaviours. For example, when the International Ski Federation issued skis of different lengths to ski-jump athletes based on athlete height and weight immediately before their jumps, there was a reduction in the percentage of underweight ski jumpers in the next world cup competition from 23% to 8%.17 The National Collegiate Athletic Association modified rules in wrestling after the deaths of three collegiate wrestlers in 199713 who were intentionally using extreme and unsafe methods to cut weight. These rule changes, reviewed by Oppliger et al. in 2006, appeared to have reduced the prevalence of potentially life-threatening practices.122 Sporting organisations should be aware of the implications of the specific rules within their sport and their potential impact on the eating practices of their athletes. It may be necessary for organisations to lobby for rule changes to decrease the risk of practices contributing to DE or EDs within their sport.
Key Points for Future Research
Further research is required in the area of DE in high performance athletes in the following areas:
- Prevalence of DE and ED in diverse population groups including males as well as females, athletes with a disability, and athletes of varying cultural backgrounds, socio-economic backgrounds and ages.
- Prevalence of athletes with LEA with and without DE or ED.
- Health and performance effects of DE on both male and female athletes. Most research in athletes is in the subspace of LEA only.
- Short and long term effects in groups of athletes using extreme dieting and DE during their sports career.
- Validated screening tools and questionnaires on DE for male and female athlete populations.
- EA assessment tools and biomarkers for early EA identification.
- Pilot prevention programs, in athletes, coaches and support staff to determine their effectiveness to decrease DE and ED occurrence.
Conclusion
This AIS-NEDC document reviews the current literature and provides a set of positions and key concepts on the approach to early identification, assessment and prevention of DE in high performance sport. Athlete health and welfare must remain the primary focus of preventing and managing DE in sport at all times. Awareness, recognition and referral of the athlete with DE to a CMT comprising a doctor, sports dietitian and psychologist forms the foundation of support for optimised nutrition. Sporting organisations should develop sport specific guidelines around DE to best optimise health and performance. This document provides guidance for the Australian high performance system to improve the awareness and management of this complex condition.